Article Text

Abstract
Objectives To identify the incidence and mechanisms of concussion in elite Field Hockey in different age groups and also the postconcussion symptoms and recovery times.
Methods Data was collected retrospectively, for both training and matches, over a 12-month period from national level Field Hockey players across under-16, under-18, under-21, Development and Senior players.
Mechanism of injury (including player role and field position), postconcussive symptoms and recovery times were recorded following a semistructured interview with each player. Additional information on training hours, matches and squad size were also recorded in order to calculate the incidence per 1000 match hours.
Results Of the 28 recorded cases, only 11 could be included in the study. Women had the highest incidence of concussion, with the majority being in the under-21 age group. Overall incidence varied from 3/1000 match hours in training to 0.02/1000 match hours in matches, with an overall incidence of 0–0.02/1000 match hours across all age groups. The most common mechanism of injury was collision with another player, followed by impact from a stick or ball Midfield and attacking forwards sustained the highest incidence of concussion. None of the concussed athletes wore protective headgear (there were no cases of concussion in goal keepers) and all occurred in open play rather than a penalty corner (when protective headgear is often worn). Postconcussion headaches and difficulty concentrating were the most commonly reported postconcussion symptoms. Average recovery time and return-to-play was 2–4 weeks.
Conclusions Due to the low numbers, only limited conclusions can be made, but it would appear that the risk of concussion in elite Field Hockey is low. As age and skill increases, the risk decreases. Postconcussion symptoms and average return-to-play times are similar to other sports. From this study, no conclusions can be made as to the role of protective headgear to reduce the risk of concussion.
- elite performance
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
The risk of concussion in elite Field Hockey is low compared with other sports.
Postconcussion symptoms and recovery times are similar to other sports.
Women report more postconcussion symptoms than men.
Average time to return-to-play is 2–4 weeks.
How might it impact on clinical practice in the future?
Is the current advice on minimum time to return-to-play too short and do we need to make this longer (minimum 2 weeks)?
Is there any need to amend the rules and/or protective headgear in Field Hockey to reduce the incidence of concussion?
Introduction
Over the past two–three decades, the game of Field Hockey has changed considerably, with the sport transitioning from being played on grass pitches to water-based artificial pitches, advancements occurring in the equipment used, players becoming substantially fitter and stronger and rule changes, such as the elimination of the offside rule, have led to Field Hockey arguably growing into one of the fastest team sports in the world.1 This ever increasing pace and intensity of the game has been suggested to lead to a higher rate of injury despite Field Hockey being shown to date as having a comparatively lower injury rate to other sports.1
Field Hockey is an extremely high paced and intense sport where the risk for sustaining a concussive injury is potentially very high. However, while a lot of awareness has been raised through the research conducted on concussion in Rugby Union, League and other sports, including Ice Hockey, little is known about concussion in Field Hockey .
The concern over sports-related concussion has been highlighted over the past decade as it may increase the likelihood of incurring a subsequent head or musculoskeletal injury and repeated concussions could be associated with long-term consequences such as persistent postconcussive symptoms, depression or neurodegenerative disorders.2
The definition of Sports Related Concussion (SRC) has been greatly debated over recent years. Following the fifth Concussion Consensus Conference in Berlin 2016, the current definition has been accepted as, ‘a traumatic brain injury that is defined as a complex pathophysiological process affecting the brain, induced by biomechanical forces with several common features that help define its nature. Limitations identified include that the current criteria for diagnosing SRC are clinically oriented and that there is no gold/standard to assess their diagnostic properties’.3
A landmark epidemiological study by Dick and colleagues4 in Field Hockey found that over the period from 1988–1989 to 2002–2003 head injuries were the only injury to increase over time, while all other injuries declined (2.5%) to the point where concussions replaced ankle ligament sprains as the most common game injury both in terms of number and rate. This was supported by a more recent study, which surveyed the injury incidence at major international Field Hockey tournaments for both men and women; the most common injury was to the head and face, making up 40% of the total number of injuries sustained in women compared with 27% in men.5 Concussions account for more than 5% of severe game injuries, with 10 or more days lost to injury, but the risk of sustaining a concussion was six times higher in a game compared with practise.
Similar findings were observed by Murtaugh in 2001,6 who conducted a retrospective analysis on the injuries sustained in women’s Field Hockey and found that concussions made up over 7% of all injuries suffered. However, neither the severities of concussion symptoms nor the types of symptoms experienced by participants were recorded, which both act as useful indicators that may influence management and in providing an approximate guideline for recovery. However, the author analysed all injuries that were reported by 158 participants and despite this large dataset, and given the confinements of the study design, provided some of the most comprehensive concussion information in the Field Hockey literature to date. The authors tried to minimise recall bias by only asking participants about the acute injuries they had experienced; however, the downside to this is that significant injuries (such as concussion) that occurred earlier in the year may have been missed.
Other studies5 7 have offered another glimpse into the incidence of head injuries in Field Hockey at international level for both seniors and juniors. However, these studies had a number of limitations, including differences in injury definition and recording and lack of differentiation between head injuries and concussion.
This study is a retrospective analysis of concussive injuries sustained by national level England and Great Britain Field Hockey players over a 12-month period with the primary objective of identifying and describing the incidence rates, mechanisms, symptoms and recovery times from concussive injuries in elite Field Hockey.
Method
This study was deemed to be of the nature of research undertaken for service improvement and so approval from an official ethics body was not actively sought. However, all players, parents, coaching and support staff were given an adult and child participant information leaflet informing them of the nature and purpose of the study in addition to a consent form which they were required to complete should they meet the inclusion criteria of the study. Prior to data collection, information was sent out to all medical personnel within the England Hockey (EH) national performance programme outlining the purpose and objectives of the study. All concussive injuries sustained during EH training camps or competitions were to be recorded on an excel database that was created and provided by the first author. The database comprises information regarding the players’ name, date on which the injury was sustained, the squad age group they were in and the primary mechanism of injury and symptoms.
Data were recorded from the period of October 2015 to November 2016, after which the database was analysed against the study’s inclusion and exclusion criterion. Participants were included in the study if they were nationally selected England or Great Britain (GB) Hockey players in the under-16, under-18, under-21, development or senior men or women squads and if they had sustained their concussion during a training session, camp or match playing for these squads. Participants that sustained their concussion during school or club matches were excluded from the final data analysis.
Further, participant information leaflets and consent forms were sent via email to participants that met the inclusion criteria to ask for their consent, or if under the age of 18 parental consent was sought, to be included in the study and contacted for a telephone interview to clarify the information regarding their injury. The telephone interview was a semistructured interview consisting of eight questions that were a mix of both open-ended and close-ended questions pertaining to the players’ mechanism of injury, location on the field of play at the time of injury, their playing position at the time, the symptoms they experienced, how long the symptoms took to resolve, the total time it took them to fully return to sport, their history of previous concussive injuries and if they had experienced any further concussive injuries between the time of data collection and follow-up. Additional information was collected from the EH performance administrator and officer for the junior and senior teams regarding the training hours, match fixtures and squad sizes for each national male and female age group in order for the exposure time during training, matches and in total to be individually calculated. It had to be assumed that each squad during training was on the field of play for 2 hours as it was not possible to accurately confirm from staff the exact time each squad was performing Field Hockey specific training on the pitch for each individual training session.
Once all data had been collected, it was analysed using an excel data spread sheet. Exposure time for each male and female age squad was calculated both for training, matches and the combined exposure time. Concussion injuries were separated into those that occurred during training versus those that occurred during matches as well as the overall rate, which was further categorised to each age group and gender. Further analysis was conducted looking into the common mechanism of injury including stick and ball contact or player collision but also whether it was a glancing blow to the side of the head or a frontal collision. This was further divided according to the players’ age squad and the player position to ascertain whether certain positions were more predisposed to concussive injury.
The location on the field of play was analysed according to whether it occurred inside the players’ circle, the 23-metre line, in the middle of the field or the opposition circle. The symptoms reported by males and females as well as the average recovery time and return to sport according to the players’ age group squad was also analysed. Finally, the incidence of concussion injuries per 1000 hours during training, match time and the combined total was calculated by dividing the total number of concussive injuries by the total exposure time and multiplied by 1000.
Results
Out of the 28 participants on the original concussion database, 22 players responded and returned the completed informed consent form. Eleven players were excluded from the final data analysis due to their concussions being sustained during either club or school matches. This left 11 total concussions that were sustained by National England or Great Britain Field Hockey players and comprises seven concussive injuries occurring to females and four to males. Under-21 women sustained the majority of these concussions during training (see tables 1–3 in the online supplementary files 1–3).
Female Field Hockey players had the highest incidence of concussion, with the majority experienced by players in the under-21 age squad with an incidence of 3 injuries per 1000 hours during training, 0.02 injuries per 1000 hours during matches and a combined total incidence of 0.1 concussions per 1000 hours. In comparison, the overall incidence of concussion both in training and matches per 1000 hours sustained by other age squads were 0.04 injuries per 1000 hours in the under-16 boy’s squad, 0.02 per 1000 hours in the under-18 men’s squad and 0.02 injuries per 1000 hours in the under-21 men’s squad (see tables 4–6 in the online supplementary files 4–6).
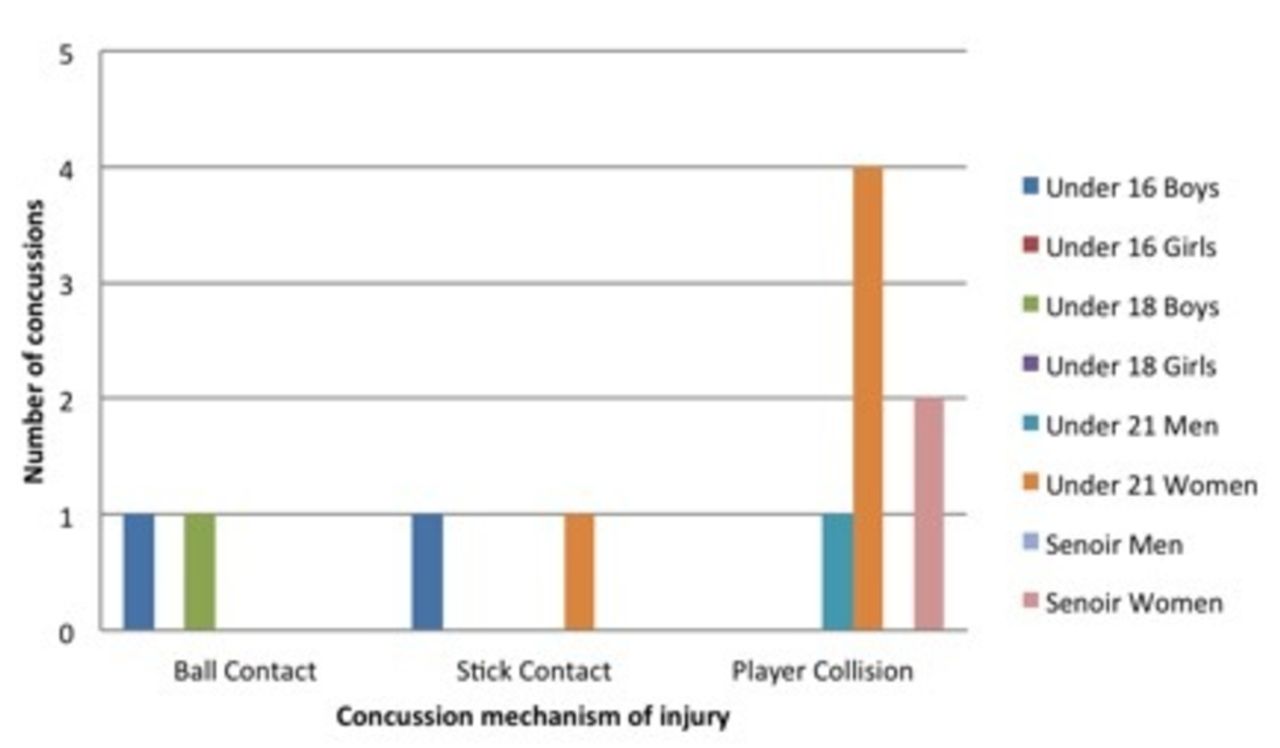
The most common mechanism of injury across all age squads and playing positions was from collision with another player, with the total incidence per 1000 hours of 0.018 versus 0.005 injuries per 1000 hours occurring from contact with either a stick or the ball. Furthermore, the most frequently cited mechanism from collision with another player was one that resulted in a blow to the side of the head, while the player was either looking at the ball or in a different direction. Midfielders and attacking forwards were the positions that sustained the highest number of concussive injuries (figures 1 and 2).

Main concussion mechanism according to age.

Concussion mechanism of injury across player positions
The majority of concussions that were sustained occurred on either the 23-metre line or the middle of the pitch, but an even split can also be seen between the injuries that occurred in the team and opposition circle. From this, however, none of the players that sustained a concussion within the circle were wearing protective headgear and all concussions that occurred inside the circle occurred during open play (figures 3 and 4).
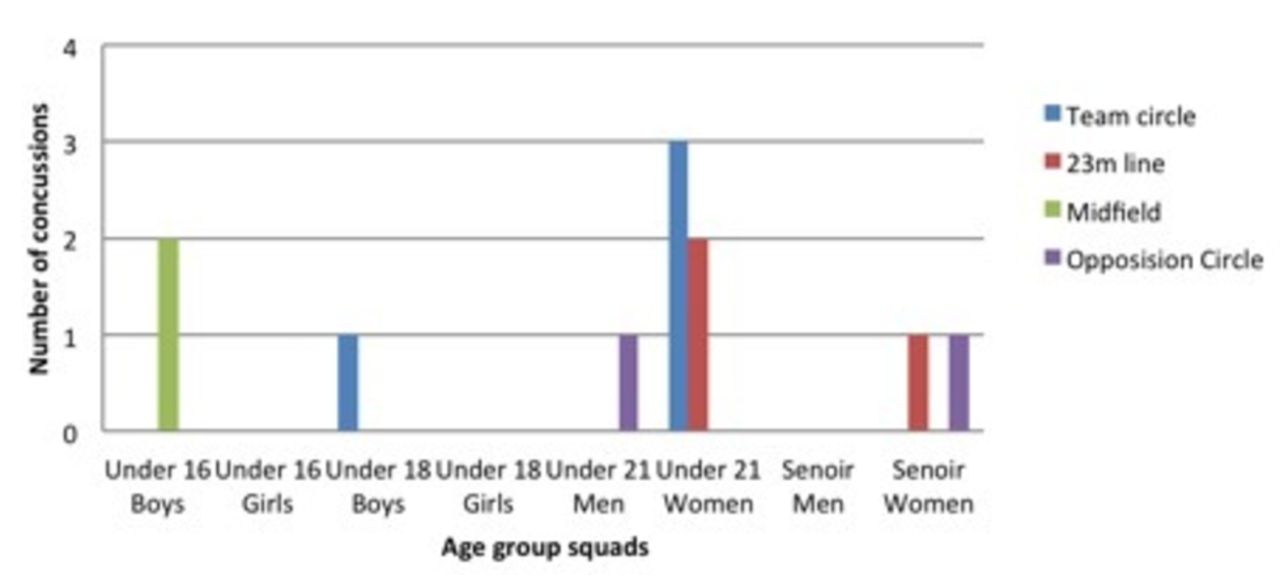
The location on the pitch where a concussion injury occurred according to age group.
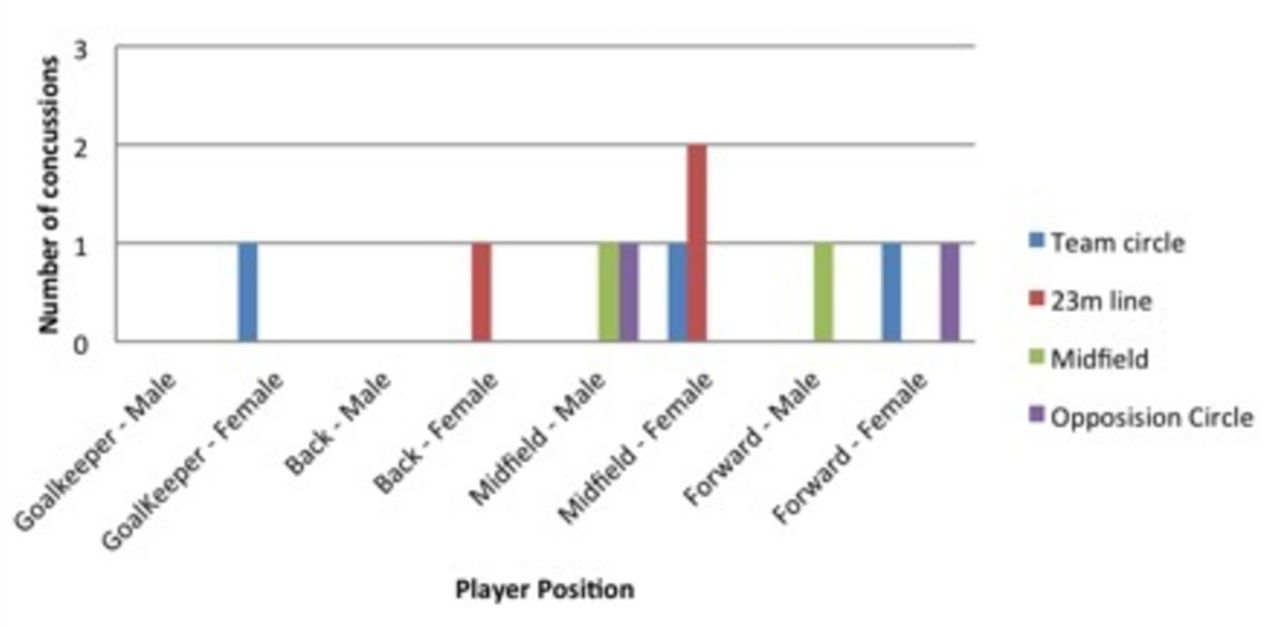
The location on the pitch where a concussion injury occurred according to player position.
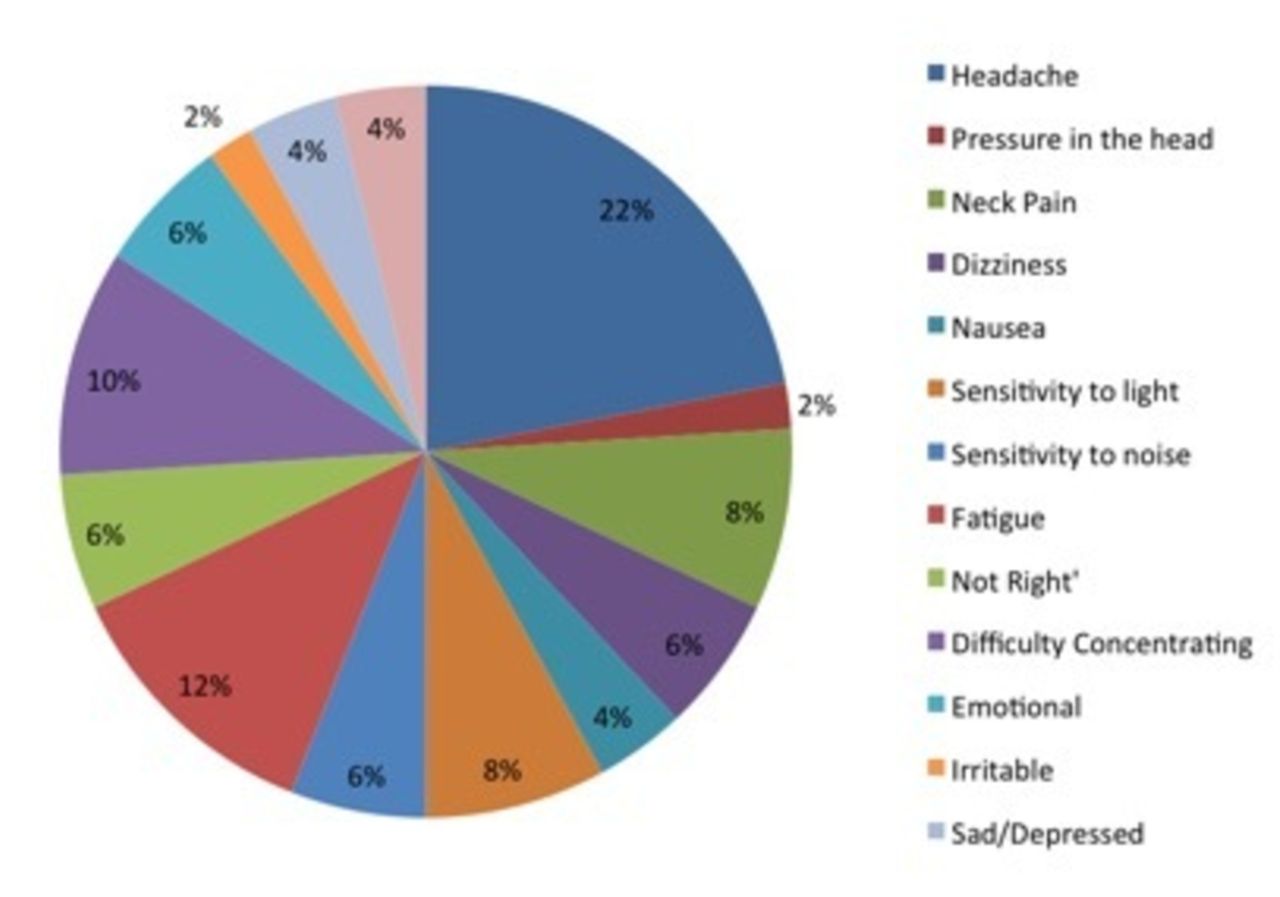
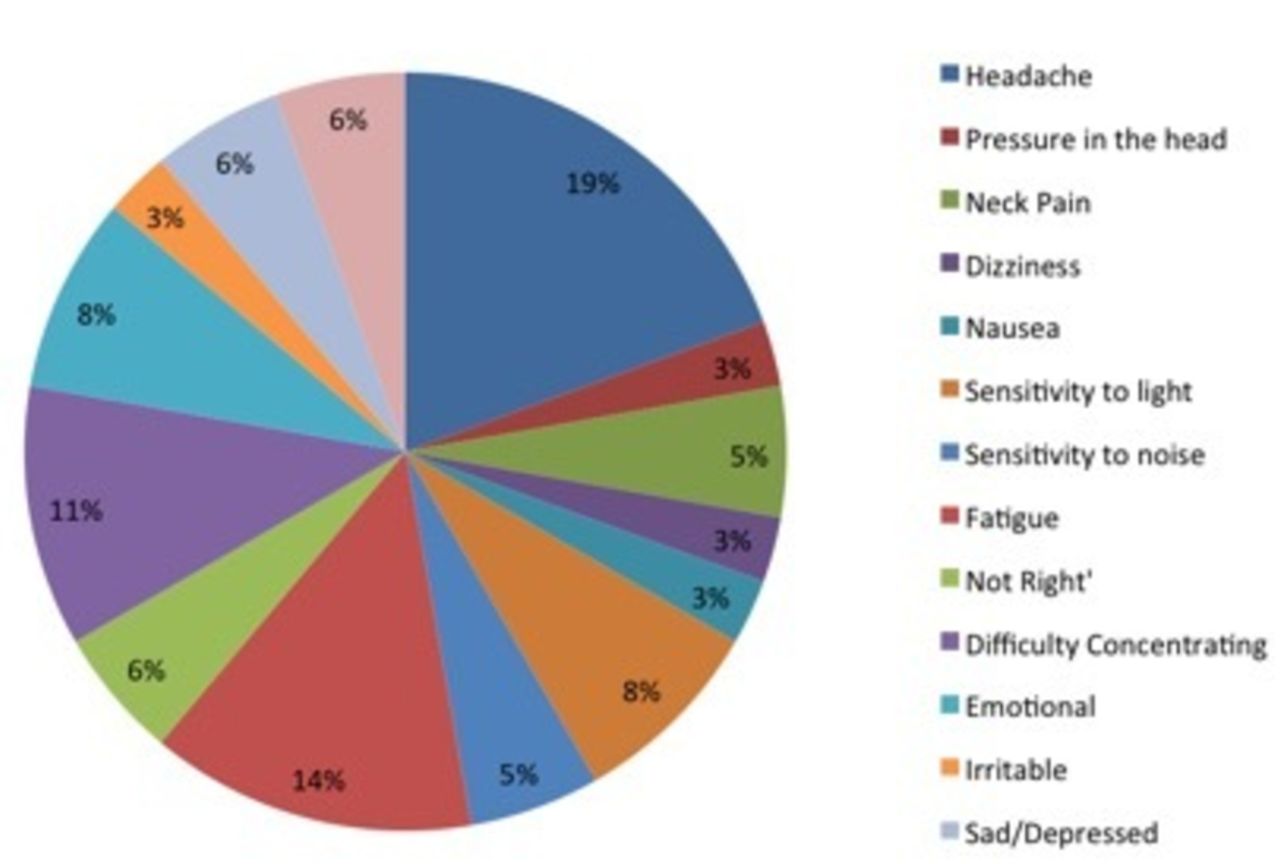
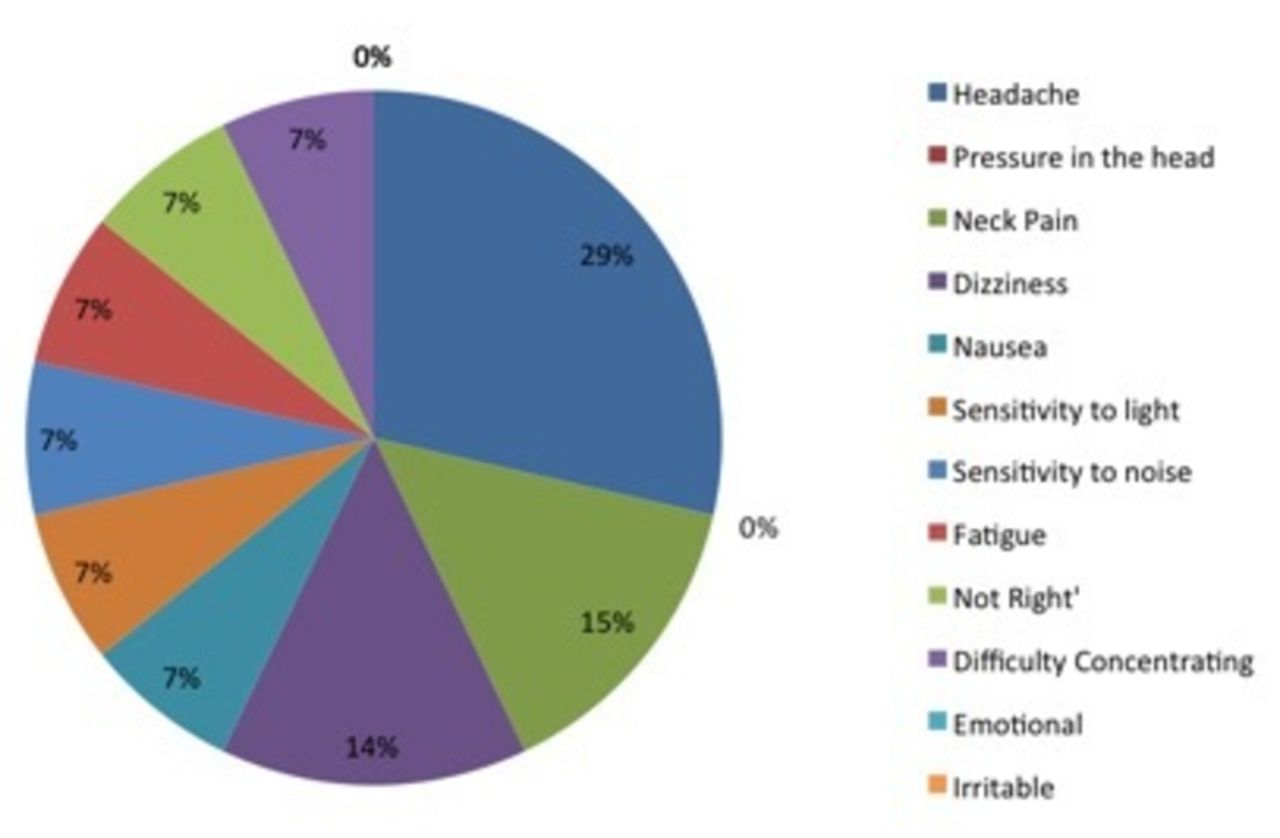
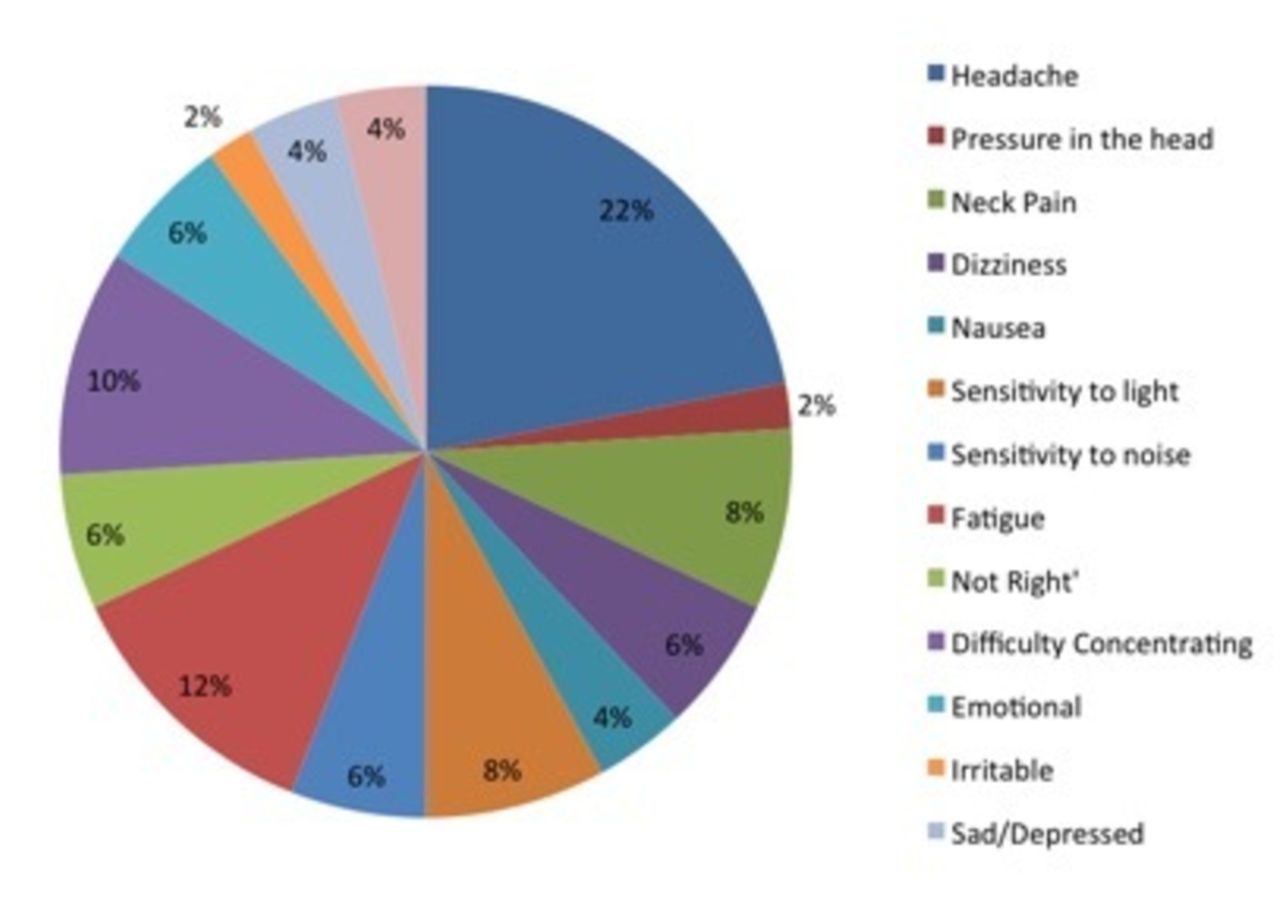
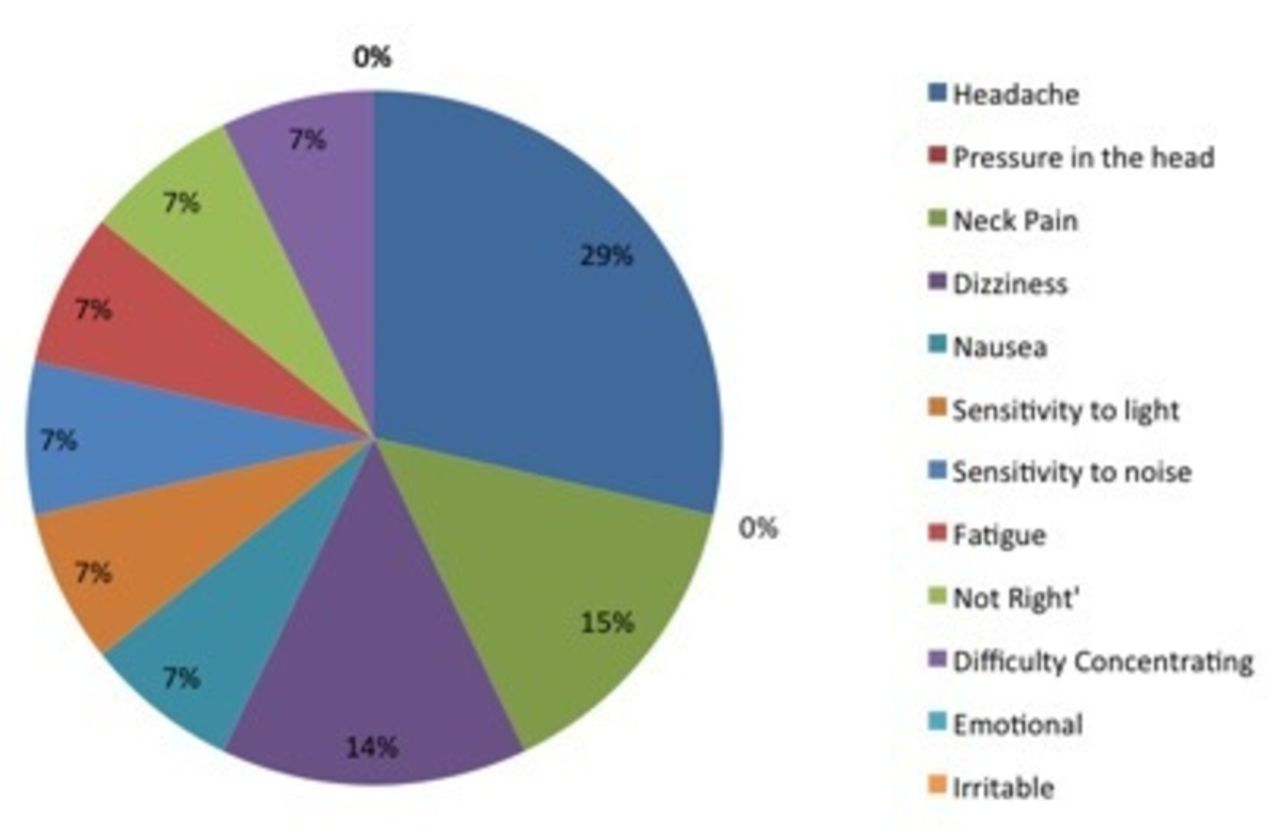
Across all age groups and genders, headache was the most reported symptom with fatigue and difficulty concentrating also being frequently stated. However, in line with the current concussion literature, there were differences between males and females, with women reporting more symptoms then men. Moreover, female players also reported higher levels of fatigue, feeling emotional, more irritable with sadness and depressive-type symptoms, whereas none of the men experienced this with their main symptoms being reported as headache, neck pain, difficulty concentrating, dizziness and fatigue. Furthermore, dizziness and vestibular symptoms did not seem to play a major role in the majority of players who sustained a concussion despite their mechanism of injury (figures 5–7).
Symptoms experienced across genders and age squads.
Concussion symptoms experienced by female hockey players.
Concussion symptoms experiences by male hockey players
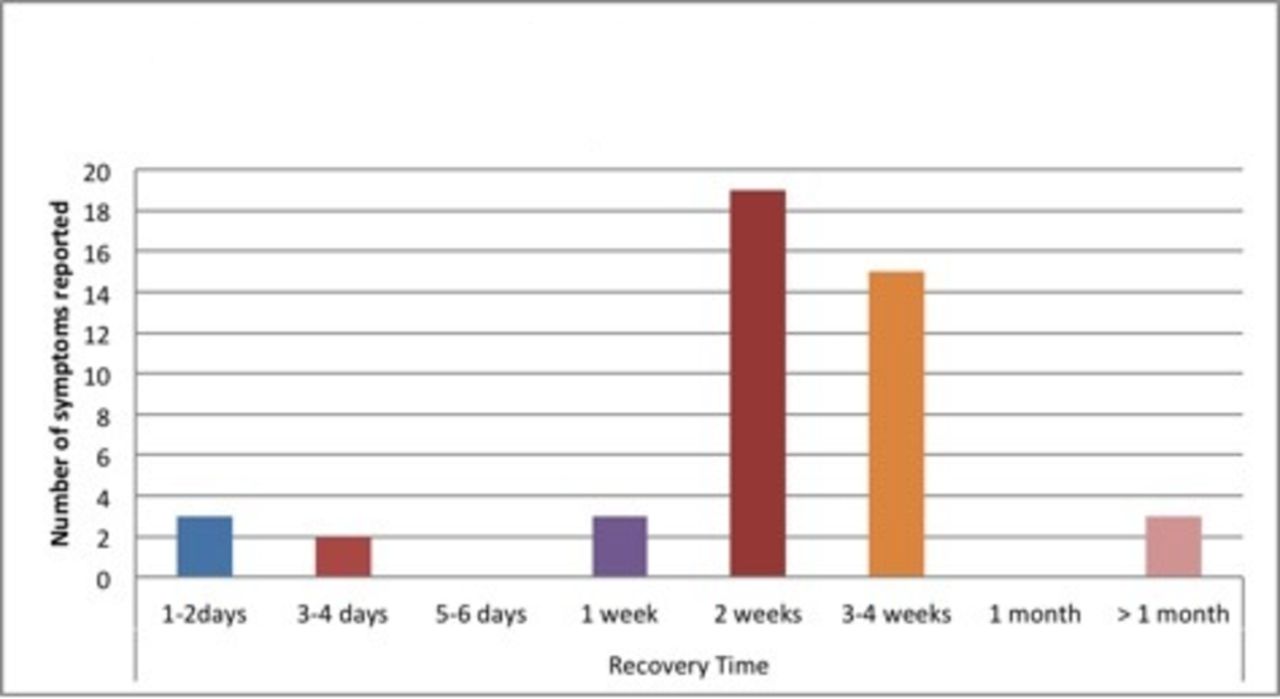
Across all age squads and genders, the average recovery time for symptoms to fully resolve was between 2 and 4 weeks and with the average time for full asymptomatic return to sport being achieved in 1 month (figures 8 and 9).

The average time taken for concussion symptoms to fully resolve.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The average time taken to return to sport following concussion.
Discussion
This current study is the first one looking at national level Field Hockey across several age groups. (The only previous study addressing concussion in Field Hockey was a Canadian study in 2015,7 which studied Collegiate, rather than elite, level players.) We draw guarded conclusions as the sample size (n=11) was very small and retrospective in nature. Our study does suggest that Field Hockey has a low incidence of concussive events, compared with other sports, with an incidence of 0.02–0.1 at under-16 to under-21 level. At senior level, the incidence appears to be rare. However, as mentioned, this may be inaccurate due to low numbers and the relatively short time period of data collection. However, overall, compared with other sports (see table 7 in the online supplementary file 7), these results suggest Field Hockey as ‘low risk’, comparable to elite level soccer8 and non-elite Australian Rules football.9
Supplementary file 4
![[SP4.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
The incidence of concussions at National level appears to increase with age, to a peak at under-21 level and then declines at senior level. There may be several reasons for this (however, larger studies need to be done to confirm this). This may include increased skill levels with increasing age; thereby the stick and ball being kept lower (although the rules state both should be below shoulder height) and better spatial awareness to avoid collisions. The peak injury rate at under-21 level may be that the game (and ball speed) is considerably faster, but spatial awareness and anticipation of potential consequences from a ‘play’ in a game, may not be as good as senior level?
The results also suggest that the incidence of concussion at elite level is lower than at collegiate level; possibly again due to increased skill and spatial awareness.
Incidence also appears to be higher in training compared with matches. Although this may be a chance finding (and small numbers), other possibilities may be a less controlled environment than a match and/or reduced player concentration in training compared with match play? Also, in younger players (under-21 and below), a far greater proportion of their ‘pitch time’/exposure comprises training as opposed to matches, whereas in senior players it was the reverse where the majority of their pitch time/exposure was spent in competitive matches.
Collision is the main cause for concussion. There may be several reasons for this. First, as mentioned, the rules of the game do not allow the ball or stick to be at head level. Also, players will follow the ball and take evasive action when possible. However, when dribbling the ball, the player has his/her head down and therefore is less aware of other players.
A blow to the side of head appears to be the most common site of injury. This may be due to the player turning their head at the point of impact to protect the face.
Midfield and attacking players were the players most at risk. This may be due to them running faster and colliding at higher speeds than defenders. Also, the attacking players tend to be smaller than their defensive counterparts, thus coming off second best in contact.
Interestingly, concussions occurring in the circle occurred only in open play and not with penalty corners. Also none of the players were wearing protective headgear at the time. This is because only defending players at a penalty corner wear protective headgear. In open play, the number of players in the circle is variable and it may be very congested, thereby increasing the risk of collision with other players, especially the goalkeeper. The ball can vary much more in its height and may be struck at high speed. At a penalty corner, the environment is different. The ball may be struck or flicked at very high speeds but the defending players are perhaps more aware and also wear protective headgear, thus reducing the risk? However, this study is too small to prove this. However, a study in the USA in 201510 looking at protective eyewear for eye and orbital injuries found that although injuries to these areas were reduced with protection, there was no significant difference in concussion rates (OR 0.77, 95% CIs and p=0.68)
Women reported more symptoms than men. There may be many reasons for this as well, such as possible under reporting by men compared with women? Also, there is a larger ball to head size ratio in women, which may be significant, as well as women having smaller neck muscle size and strength.11 Women also report more emotional labiality and fatigue compared with men. This may be due to differing perception of symptoms and/or underreporting by men. Also, the role of oestrogen, increased cerebral blood flow and glucose metabolism have also been implicated.11 12 Men reported higher levels of headache, neck pain and dizziness, which may reflect the possible increased impact compared with women from increased collision speed, speed of ball or stick, all causing increased cervical rotation and/or vestibular involvement. The reported symptoms by both men and women (neurological, oculomotor, visual, neurocognitive, psychological and cervical) are similar to those in other sports and are now recognised as being important in the assessment of Sports Related Concussion.13 Although age, sex and sport may influence the results, the recommendation now is that consensus-derived multimodal assessment tools (such as Sports Concussion Assessment Tool (SCAT)) should include these symptoms. Sideline video may also improve recognition and removal of players and there may also be a place for oculomotor tests (such as the King-Devick Test), although this is still under review.2 14
Average recovery times were 2–4 weeks with full resolution occurring at 4 weeks. This is similar to studies in other sports and also across different age groups,15–20 which raises the question regarding return-to-play. For England and GB Field Hockey, currently any player over 18 years old can return to play within 7 days if they are asymptomatic and return to at least their baseline SCAT 3 levels.21 However, does this study suggest that 7 days is too soon for some, or even most, players? Once again, larger studies looking at return-to-play need to be done.
Conclusions
Due to the small numbers and retrospective nature of this study, only limited conclusions can be drawn and larger, longer and more specific studies need to be conducted in Field Hockey. However, compared with other sports, the risk of concussion in Field Hockey is low. It also suggests that as age, and possibly, skill level increases, the incidence of concussion decreases, despite the increased speed of the players and ball. This may be due to better spatial awareness and therefore fewer collisions with other players.
The postconcussion symptoms and recovery times were similar to other sports which raise the question of when is it safe to return-to play, as 7 days may not be enough.
No firm conclusions can be made regarding protective headgear in/out of the circle or any need for rule changes.
Supplementary file 7
![[SP7.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Supplementary file 1
![[SP1.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
Supplementary file 2
![[SP2.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Supplementary file 3
![[SP3.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
Supplementary file 5
![[SP5.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Supplementary file 6
![[SP6.jpg]](https://bmjopensem.bmj.com/content/bmjosem/3/1/e000260/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
References
Footnotes
Contributors Reporting of concussive incidents was made by Physiotherapists or Doctors attached to each national age-group squad. The planning of the study was done mainly by the first author. The consenting, interviewing and outcome data were collected by the second author. The conclusions and final editing of the study was by the first author.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Open access is available for all data.