Article Text

Abstract
Objective Physical activity is important for well-being but can be challenging for people with diabetes. Data informing support of specialist activities such as climbing and high-altitude trekking are limited. A 42-year-old man with type 1 diabetes (duration 30 years) attended a Multidisciplinary Physical Activity and Diabetes Clinic planning to climb Mont Blanc during the summer and trek to Everest Base Camp in the autumn. His aims were to complete these adventures without his diabetes impacting on their success.
Methods We report the information provided that enabled him to safely facilitate his objectives, in particular, the requirement for frequent checking of blood glucose levels, the effects of altitude on insulin dose requirements, and recognition that acute mountain sickness may mimic the symptoms of hypoglycaemia and vice versa. Real-time continuous glucose monitoring was made available for his treks.
Results The effects of high altitude on blood glucose results and glycaemic variability while treated on multiple daily injections of insulin are reported. In addition, we present a first-person account of his experience and lessons learnt from managing diabetes at high altitude.
Conclusions A dedicated Multidisciplinary Physical Activity and Diabetes Clinic delivering individualised, evidence-based, patient-focused advice on the effects of altitude on blood glucose levels, and provision of real-time continuous glucose monitoring enabled uneventful completion of a trek to Everest Base Camp in a person with type 1 diabetes.
- diabetes
- glucose
- mountain
- walking
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Mountaineering and high-altitude trekking are popular pastimes.1 Altitude can cause either hypoglycaemia or hyperglycaemia in trekkers and climbers with diabetes. There is limited rigorous evidence to assist people with diabetes in managing their blood glucose while exercising at high altitude (although there is plenty of research regarding glucose metabolism in people without diabetes). Nevertheless, there are several excellent review articles available.2–5 Sustained physical activity has benefits on mortality for people with and without diabetes.6 Less studied but equally important are the non-tangible benefits from taking part in physical activity and sports— satisfaction, camaraderie and friendship. The American Diabetes Association advocates that people with type 1 diabetes should be able to partake ‘in all physical forms of activity consistent with an individual’s desires and goals.’7
Methods
We have established a Multidisciplinary Physical Activity and Diabetes Clinic, aiming to empower, educate and enable people with diabetes to undertake sports, activity and exercise unimpeded by glycaemic variability and injuries. The clinical team include a diabetologist, diabetes dietitian, diabetes specialist nurse and consultant in sports and exercise medicine. In 2016, a 42-year-old man (GM) who had had type 1 diabetes for 30 years attended with the intention of climbing Mont Blanc (4800 m) in the summer and trekking to Everest Base Camp (5300 m) then summiting Kala Patthar (5600 m) in Nepal during the autumn. To facilitate this, he assiduously prepared for these trips and we provided real-time continuous glucose monitoring (CGM) (Dexcom G4, San Diego, California) to support blood glucose self-management. In addition, we synthesised the available research information into a reference document/factsheet designed to support his preparation and planning (box 1). His pre-trek insulin regimen was insulin glargine (Lantus, Sanofi, USA) 22 units in the morning and 15 units in the evening; he counted carbohydrate for administration of prandial insulin aspart (NovoRapid, Novo Nordisk, Denmark). His pre-trek GOLD score was 3, indicating intact awareness of hypoglycaemia. His BMI was 27.3 kg/m2.
Advice for people with diabetes intending to undertake a trek or climbing expedition to high or very high altitude
Recommendations for people with diabetes planning to trek/climb at altitude
High (3000–5000 m) and extreme (>5000 m) altitude can result in hypoglycaemia and hyperglycaemia in trekkers and climbers with diabetes, depending on the rate of ascent and altitude attained.4 5 8 This is thought to be, in part, due to reduced food intake and delayed absorption of carbohydrate at mealtimes, as well as high levels of exertion and increased anaerobic exercise.2 8 Some studies have shown that at altitude insulin requirements may need to be reduced by up to 50%, whereas others have shown increased insulin requirements at extreme altitude perhaps due to altitude-induced increases in counter-regulatory hormones.4 5 9 At high altitude, insulin requirements are affected by factors that cause hypoglycaemia (exercise, reduced dietary intake) and factors that increase blood glucose levels (short intense exercise, stress or acute mountain sickness (AMS) giving raised counter-regulatory hormones).2 3 Thus, maintaining stable blood glucose levels requires great deal of trial and error, acquisition of experience, and will depend on altitude and exertion. An understanding of carbohydrate counting is likely to be an advantage when climbing and trekking at high altitude and we suggest this is undertaken or revised prior to departure. In addition, frequent monitoring of blood glucose levels will help identify unexpected changes.
It has been reported that although insulin requirements may rise due to increases in counter-regulatory hormones, diet and exercise actually have a greater effect on blood glucose levels than high altitude itself.10 Loss of appetite at high altitude is common. At extreme altitude, slowing of food absorption has (in some cases) led to hypoglycaemia after meals with subsequent hyperglycaemia, suggesting that above these elevations, bolus insulin may be better taken with or even just after a meal, rather than the usual before-meal dosing.2 5 8
When climbers are at high altitude, appetite appears to be suppressed and fewer calories are consumed (although energy expended for the same amount of work does not change at high altitude).2 11 However, the palatability of sweet foods remains unaffected at altitude, even with AMS, and snacks with high carbohydrate content should be available for people with insulin-treated diabetes who are trekking at altitude to sustain energy and prevent hypoglycaemia.
The potential for high altitude and extreme temperatures to affect the reliability and accuracy of blood glucose metre readings means climbers with diabetes should be cautious about how they interpret their blood glucose results.3 5 Most modern metres work between 10°C and 40°C and may not work reliably outside of these ranges. In some cases, warming a glucometer that has stopped functioning using body heat will resurrect it, but the reliability immediately following this is not known. There is some suggestion that meters that use glucose oxidase-based enzyme reactions on their testing strips may over-read blood glucose readings due to the low blood oxygen tension compared with glucose dehydrogenase-based testing strips.3 However, other studies have shown the opposite at moderate altitude.2 Checking which blood glucose metres are approved for high-altitude travel is recommended, and we suggest using standardised solutions to calibrate the machines and to help understand the variation and biases that occur.12 It is also worth remembering that aspirin and paracetamol can interfere with the reliability of blood glucose readings. In addition, we suggest that ‘sick day rules’ are reviewed as part of predeparture preparation, especially regarding the management of illnesses that induce nausea or vomiting, which may occur in AMS, diabetic ketoacidosis (DKA) or gastroenteritis, all of which would not be unexpected while trekking at high altitude. In brief summary, these involve taking regular blood glucose (and if appropriate, ketone) measurements and never stopping insulin when unwell.
There is no apparent increased risk of AMS in people with diabetes compared to those without.2 It is recommended that if preventive medications are used to assist acclimatisation, dexamethasone (a steroid) is avoided due to its effect on increasing insulin resistance and increasing blood glucose. If acetazolamide (Diamox) is to be used for AMS prophylaxis, then this may cause both increases and decreases in blood glucose and therefore if its use is contemplated for this purpose, a therapeutic trial before departure, with appropriate insulin dose adjustments, is recommended. The use of acetozolamide has been associated with DKA in some climbers with diabetes so it should be used with considerable caution, after discussion with a doctor.5 13 The symptoms of AMS may mimic those of hypoglycaemia, so again, frequent blood glucose monitoring is really important.
Other considerations:
It is important to ensure that insulin does not freeze (ideally it should be stored between 2°C and 8°C). Using body warmth can prevent insulin (and glucose metres and batteries) from freezing, by storing in pouches in internal pockets or even building home-made pouches from fleece-like materials to store just outside the base layer of thermal underwear. Keeping these items at the bottom of sleeping bags overnight is also worth considering. Similarly, others have recommended keeping insulin wrapped in bubble wrapping inside a vacuum flask. If you have unexpectedly high blood glucose levels, try using a new insulin pen/cartridge in case the current one has been affected by cold.
Managing hypoglycaemia is clearly important and it is suggested that glucogel and/or glucagon are available and carried in a pocket that is easy to access. Be aware that glucagon may be ineffective after significant exercise because the body’s glycogen stores (which are released by glucagon and converted to glucose) may be depleted. A companion should be informed about where these are kept and how to use these in the event of significant hypoglycaemia.
High-altitude retinal haemorrhage is a recognised condition and there is a theoretical risk of worsening of diabetic retinopathy at altitude.5 Retinal screening or fundoscopy by your doctor or optician is recommended prior to departure.
Carry spare supplies of everything related to your diabetes; one set should be on your person and the other with your kit.
Many other resources are available, for example, Mountains for Active Diabetics: www.facebook.com/groups/131297830871/ and www.runsweet.com/diabetes-and-sport/high-altitude-trekking/
Results
GM describes his experiences (box 2). The day of trek, activity or trekking destination, and sleeping altitude are described in table 1. The CGM data from the Everest Base Camp trek that GM undertook (table 2, figure 1) show that the mean CGM glucose measured over 14 days before the trek was 8.7 mmol/L, during the trek it was 10.8 mmol/L, and after the trek it was 10.1 mmol/L. This reflects GM’s pre-trek intention, which was to avoid hypoglycaemia at altitude; this was achieved by reducing his basal insulin dose from 22 to 20 units and reducing his insulin to carbohydrate ratios. The amount of time with glucose between 3.9 and 7.8 mmol/L decreased, and the time with glucose levels above 15 mmol/L also increased from less than 2% pre-trek to more than 10% during the trek. Whether this relative increase in overall glucose affected performance is not clear. We also report markers of glycaemic variability before, during and after his trek (table 3); interestingly, these markers do not differ much between the pre-trek, trek and post-trek periods.
Personal experience of a 42-year-old man with diabetes undertaking a trek to Everest Base Camp, Nepal, in 2016
How a person with type 1 diabetes successfully trekked to nearly 6000 m in Nepal
Before Nepal:
Long before my Nepal trip (October 2016) I undertook a number of activities to become fitter that I felt could improve the chances that I would cope with the demands of trekking at the high altitudes of Nepal. In January 2016, I started to measure my weight (about 12 stones), daily steps and calories I gained or lost on a daily basis, to help reduce my weight so that I could reduce the pressure on my knees. When I left for Nepal I had lost a stone in weight.
These activities included:
Set, and met, daily targets to walk at least 15 000 steps (measured with my Fitbit).
In July I climbed Gran Paradiso in Italy (4061 m) but failed to summit Mont Blanc (the highest mountain in Western Europe, 4809 m) when I suffered from altitude sickness at around 4200 metres.
Took part in weekend hikes of varying difficulties. Some as short as 7 miles and some as long as a hilly 15 mile walk.
The result of these preparation activities was to increase my general fitness and my HbA1c reduced to 56 mmol/mol in August (it was 63 mmol/mol in February).
Lessons learnt:
After failing to reach the summit of Mont Blanc, I wanted to ensure I did not suffer in Nepal with altitude sickness (on Mont Blanc I totally lost my appetite) as this would cause problems with my diabetes management. The areas I looked to make changes were:
I ensured that I drank at least two litres of water a day but always added electrolyte packs so that I had enough salts and minerals in my system as well. During my activity in the Alps to ascend Mont Blanc, I observed that I was thirsty more than in other similar mountaineering experiences and this was when my blood sugar readings were much less consistent (often higher than usual).
On Mont Blanc it was often too cold for my blood glucose meter (Accu-Check) to work so I needed to find an alternative for Nepal as the overnight temperatures were expected to be anywhere between −5C to −20C.
In Nepal
When I landed in Kathmandu, Nepal (1400 metres) I noticed that the delay between giving my fast-acting insulin and my blood sugars reducing, was consistently increased by 20 min. I knew this could occur in people with diabetes at higher altitudes but was surprised it affected me at this early stage in the trek.
The flight to Lukla was quick and took me up to 2800 metres where the accommodation was in tea houses (wood homes where pairs shared rooms). There was no heating and electricity (lights) in the rooms was only present in the late afternoon and evenings. At night head torches were needed to visit the toilets. In Nepal during October and early November at 6 am in the morning it was very cold and sunny; the mornings and early afternoons were often very warm, and at 4 pm it became cold and the wind bit somewhat. We had no access to fridges during the trek and so I had to do the best as I could to store insulin. When we moved between tea houses on the approach to, and return from Everest Base Camp, insulin for immediate use was carried in my day bag to avoid direct sunlight, limiting temperature changes. I also stored a supply in the bags that the Yaks carried (again to block any direct sunlight) but also to ensure I did not have all my eggs in one basket—ie, lose a bag and so have NO insulin.
Speaking to the tour manager, I followed a few additional pieces of advice to avoid other illnesses:
Never take water from the taps due to the high risk of stomach bugs. Using sterilisation tablets was an alternative but I tended to find that the bottled water was available almost everywhere and was very cheap (unlike in the Alps).
Use an anti-bacterial hand wash every time you go to the toilet, touch surfaces, before and after eating food (pretty much everywhere) to reduce the chances of catching a bug.
I ate no meat on the trek (I am not vegetarian), again to reduce the chances of catching a stomach bug.
I drank no alcohol on the trek (apart from the last two days when back in Kathmandu).
The next couple of days involved a trek to Phakding (2600 metres) and then we ascended steeply to Namche Bazaar (3400 metres) crossing many large suspension bridges. At this point walking at the increased altitude was not overbearing but it became important to monitor my blood sugar levels and the direction of travel (rising or falling) so I could eat enough food to ensure my blood sugar did not rise too much, or fall below 6 mmol/L. In this first week of the trek it was difficult to do this because in the UK my blood sugar usually rose throughout the morning (I have an office based job) and in Nepal it meant that I tended to give less fast acting insulin—the walking caused it to be steadier rather than to rise. Getting this balance was not easy, as each day the gap between breakfast and lunch was different—in part because the group would sometimes wait for those nearer the back of the 20 trekkers to catch up (4 guides plus 16 tourists). In terms of food it would be expensive to buy in Nepal so I brought with me a range of sugary snacks—some dextrose energy tablets and other cereal based snacks to give a longer-term carbohydrate.
During the trek, I made use of a real time continuous glucose monitoring (Dexcom G4) and used my conventional blood sugar meter to calibrate the real-time reader. Whilst on Mont Blanc, often my standard blood reading machine would not work whereas in Nepal the CGM was available all of the time. The aspect of only needing to calibrate it twice a day meant that I did not need to rely on my traditional machine as often but when I needed to calibrate the CGM (using my usual blood sugar reader) I could choose to do so by wrapping my machine in my hat/warm clothes/next to body so it would work during the calibration process despite the difficulties of having to keep it warm.
Once I realised that each tea house had an almost identical menu I decided to have the same breakfast everyday (white coffee plus one fried egg and two rounds of toast). This allowed me to help stabilise my blood sugar levels in the morning as well as measuring the effect of changing insulin regimes during different times of the day.
The next part of the trek was an acclimatisation walk to Kunde (3800 metres), Khumjung (3800 metres) and then to Kyanjuma (3500 metres) so we would be in a better shape for when we approached Base Camp. At this time, I altered my evening slow acting insulin. The 14 units I usually took at 11 pm before bed in the UK was replaced by 10 units at 9 pm to ensure I did not repeat a couple of the minor hypoglycaemic attacks that I had in the first week. This meant I woke with slightly elevated blood sugar levels but I generally dealt with this by giving a little more correction at breakfast, so as the morning wore on my blood sugars were more consistent.
Trekking to Thyangboche (3900 metres) was where the temperature became noticeably colder at night. I kept batteries and blood sugar readers in internal pockets and inside my sleeping bag (to prolong their life) as charging points were very expensive. I noticed that two of the Dexcom sensors had their transmitter latches snapped off (probably due to being carried in the bag which was carried by Yaks).
The next day was an acclimatisation day at Dingboche (4400 metres, the highest altitude I had been to) but this time I felt healthy, was eating every meal and was not struggling to breathe. At this point two trekkers in the group were sick with stomach issues and diarrhoea. My blood sugar levels but did not show unexpectedly increased readings—a sign I may have caught an illness. Phew!
I tended to change foods I ate in the evenings each day so that I would not get bored. However, on advice from the tour manager to help reduce the chance of suffering from altitude sickness, I ate garlic soups as well as drinking lemon and honey tea (although there is no published evidence that these are effective in preventing AMS).
With the environment lacking trees and the wind becoming stronger, we walked faster to get to the next stop. Storage of the insulin was okay but injecting the insulin gave me a sharp cold feeling as it was dispensed under the skin. On that day, two people left the trek due to altitude sickness and were taken to a village where we would later meet up with them on our return from Everest Base Camp. We continued our ascent to Lobuje (4900 metres) and in the evening, some of us took oxygen saturation measurements using a device two of the group had brought. I registered 93% on that day and the same the following day which was the highest in the group. I was equal with the Lead Sherpa who came from Nepal which showed my pre-trip training was working.
On the next day, one person's illness had improved and another person was unwell, but I remained okay. The group arrived at Everest Base Camp (5300 metres) and spend the night at Gorak Shep (5100 metres). One of the group needed oxygen because his oxygen saturation was circa 40%. He made it to Gorak Shep, looking weaker than we had seen him before. Overnight it was −20°C in our room and using my standard blood glucose meter was not possible, even when taking it from my sleeping bag and being covered in a woolly hat. My blood sugar readings seemed to be more consistent than the previous week.
Whilst I was at more than 5000 metres altitude, the delay between giving my fast-acting insulin injection and a reduction in blood sugar was about 3 hours. This meant that as the altitude increased I needed to inject earlier than I would normally (more in advance of meal time). I was nervous at first but this was a requirement to avoid constant high blood sugars.
The next day I got up a lot earlier (at about 4 am) so four of us could climb Kala Patthar (5600 metres). Because this was going to be a long day I chose to administer my morning long acting insulin when I had climbed Kala Patthar, so that the time I gave it would be similar to previous days. This worked well and when two of us had summited Kala Patthar we (and the other two who had stopped short of the summit), ate breakfast (albeit a little later than previous days).
We descended to Pheriche (4400 metres) and then the pace of decent became faster as we headed to Lukla (2800 metres) via Kyanjuna (3800 metres) and Phakding (2600 metres). On the last section to Lukla my real time CGM showed my sugar levels of falling sharply. I ate a number of sugary bars and when that did not stop the fall quickly, I stopped to rest. After about thirty minutes my blood sugar levels had fallen to below 3 mmol/L and then rose to about 8 mmol/L before I set off slowly (this section was a very slight rise). I could not identify why my blood sugar had fallen as I had not eaten any less than normal or trekked longer (only perhaps quicker) but perhaps the lower altitude caused the previous fast acting insulin injection to act more quickly than on previous days. I flew to Kathmandu where I had a celebratory drink. I did notice that a single can of beer had the effect of me being light headed (not the usual case in the UK)!
In summary, I would say that I prepared well and this allowed me to understand my body enough that I could make changes in unknown situations to keep my blood sugars reasonably consistent and not at too high a level.
Top Tips
My main tips for maintaining blood sugar levels at high altitude are:
Try to keep blood sugar levels at around 9 mmol/L, which will give you some leeway whilst trekking.
Consider altering your morning or evening boluses of long acting insulin. Use the first week to measure to blood sugar levels and make alterations for the second week based upon this knowledge.
Carry unused Dexcom Sensor packs with you to reduce the chance of the transmitter latches being broken off in transit.
Take lots of types of snacks with you, so you can better maintain your glucose levels.
Lastly, inform other trekkers and the tour organisers that you have diabetes and what symptoms to look out for, and how to deal with them.
Activities and trekking destination (with sleeping altitude) during a trek to Everest Base Camp in the Himalayas
Continuous glucose monitor readings, shown as a per cent of total readings before (pre-trek, 3908 readings), during (trek, 4976 readings) and after (post-trek, 3866 readings) a trek to Everest Base Camp by a 42-year-old man with type 1 diabetes. Pre-trek and post-trek altitudes are at sea level

{kind=link}
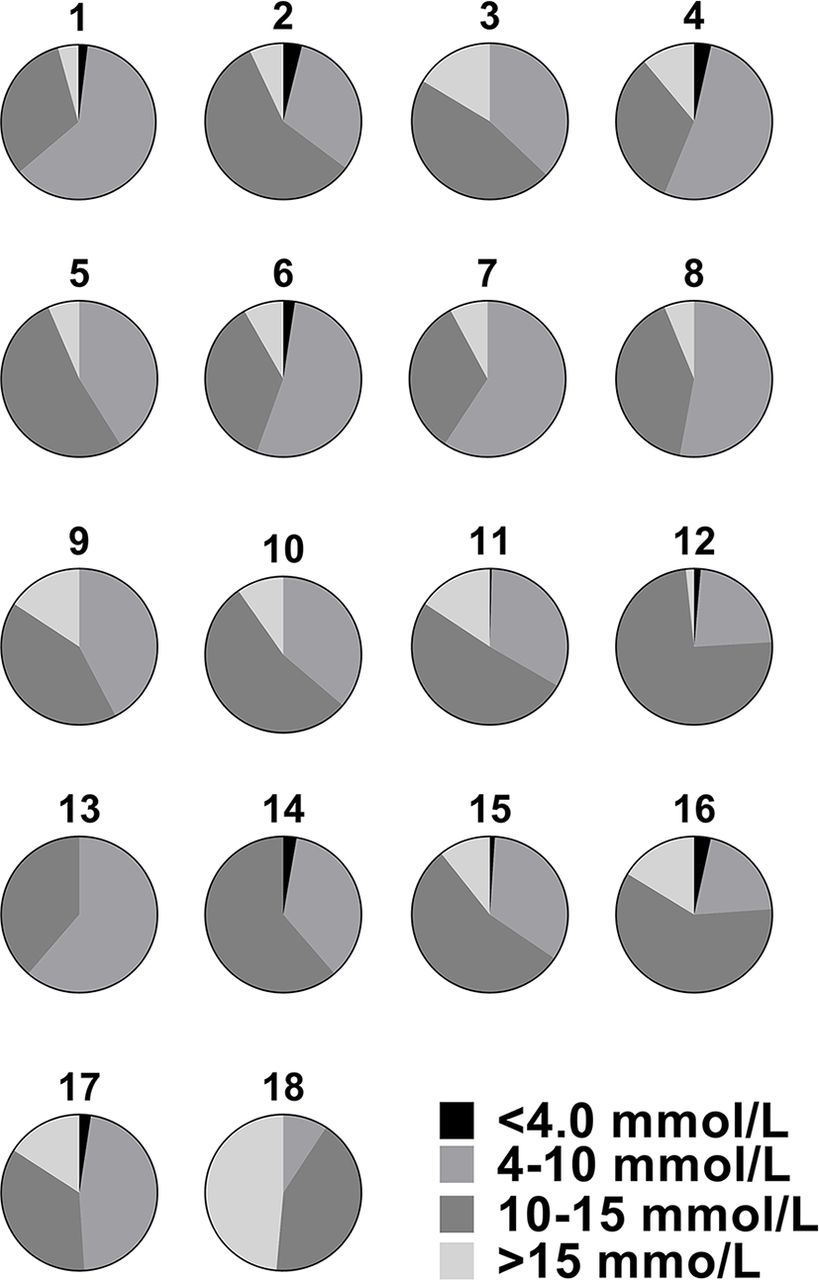
Continuous glucose monitor readings during a trek to Everest Base Camp shown as a per cent of total readings with CGM glucose below 3.9 mmol/L, 3.9–10 mmol/L, 10–15 mmol/L and more than 15 mmol/L for each day (Days 1-18, correlates with location and sleeping altitude in table 1). CGM, continuous glucose monitoring.
Markers of glycaemic variability before (pre-trek), during (trek) and after (post-trek) a trek to Everest Base Camp by a 42-year-old man with type 1 diabetes. Pre-trek and post-trek altitudes are at sea level
Discussion
We present a case report of high-altitude trekking in type 1 diabetes. The preparation and support provided, including CGM technology, enabled safe travel to above 5000 m where changes to physiology and metabolism are associated with challenges to self-management. The first-person narrative provides additional information on the issues of self-management for people with type 1 diabetes. The case emphasises the importance of multidisciplinary support for physical activity and exercise in people with diabetes, and the potential benefits of adjunctive technologies. By adjusting his insulin doses and using CGM readings, GM was able to avoid hypoglycaemia. This was done at the expense of higher average glucose readings during the trekking period, by following the pre-trek advice and using the experience of having had diabetes for 30 years plus that of his Mont Blanc trip and that gained while in Nepal. His assiduous preparation meant that there were no diabetes-related issues that compromised him during the trek. It seems that while it is important to provide supporting information for people wishing to undertake climbing and trekking at altitude (and indeed any sport or exercise), learning from personal experience is a key factor in the success of any formalised physical activity.
Although we have experience of using diabetes technology at altitude, the clinical team have no direct experience of managing diabetes at very high altitude and used published data to assist preparation for this trip. Further information on the accuracy of CGM and handheld glucometers at high altitude and the effects of altitude on glycaemia in free-living people with diabetes is required.
Summary
People with diabetes can undertake demanding arduous physical challenges unimpeded by significant unwanted glycaemic excursions (in particular hypoglycaemia) with adequate planning and preparation, which may be facilitated by their clinical team.
The effects of ascent to high altitude on blood glucose levels are variable and insulin doses may need to be adjusted. Real-time continuous glucose monitoring can be used to assist insulin dose adjustment.
A Multidisciplinary Physical Activity and Diabetes Clinic can enable, educate and empower people with diabetes to attain their objectives through enhanced self-management of diabetes before, during and after physical activity.
Footnotes
↵* GM contributed to this article but is not affiliated with an academic institution.
Contributors GM wrote the first person account part of the manuscript, undertook trek. SR and CJ contributed to the trekking advice part of the manuscript, advised GM. SS and NO undertook the analysis of CGM, contributed to the trekking advice part of the manuscript. SC contributed to the trekking advice part of the manuscript. NH coordinated and wrote the manuscript, advised GM.
Competing interests NO has received honoraria for advisory board membership from Roche and Abbott Diabetes. NH has received continuous glucose monitoring equipment from Dexcom (San Diego, California) for research.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.