Article Text

Abstract
The nomenclature and the lack of consensus of clinical evaluation and imaging assessment in groin pain generate significant confusion in this field. The Groin Pain Syndrome Italian Consensus Conference has been organised in order to prepare a consensus document regarding taxonomy, clinical evaluation and imaging assessment for groin pain. A 1-day Consensus Conference was organised on 5 February 2016, in Milan (Italy). 41 Italian experts with different backgrounds participated in the discussion. A consensus document previously drafted was discussed, eventually modified, and finally approved by all members of the Consensus Conference. Unanimous consensus was reached concerning: (1) taxonomy (2) clinical evaluation and (3) imaging assessment. The synthesis of these 3 points is included in this paper. The Groin Pain Syndrome Italian Consensus Conference reached a consensus on three main points concerning the groin pain syndrome assessment, in an attempt to clarify this challenging medical problem.
- Groin
- Hip
- Muscle injury and inflammation
- Sport
- Tendinopathy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Groin pain (GrP) is a widely recognised medical issue among professional and amateur athletes. It is a very significant injury, associated with major time loss from sports, and can sometimes be a career-ending injury. It is important to point out that the term ‘groin pain’, and also all the other terms that are used worldwide describing the same symptoms, such as athletic groin, groin disruption, sportsman's groin, sportsman's hernia, athletic pubalgia, etc, are descriptive, and describe ‘pain in the groin area’, which cannot be a diagnosis. In fact GrP, and in special manner chronic GrP, has a multifactorial pathogenesis and often different pathologies overlap becoming, sometimes, a real diagnostic challenge. Objectively the anatomical complexity of the pubic region certainly does not facilitate the adoption of a clear terminology. In the current literature, one of the most rational GrP classifications is proposed by Omar et al.1 In this classification, the diagnosis is based on 37 major diseases grouped into 10 categories. Following this first classification, the British Hernia Society had a consensus meeting in 2012, with a position statement on GrP2 which focused mainly on inguinal canal pathologies, and proposed the term ‘inguinal disruption’ for describing athletes with ‘groin pain predominantly in the groin area near the pubic tubercle’. More recently, it is important to note the conclusions reached during the 1st World Groin Pain Conference in Doha, Qatar, in November 2014, followed by the Doha Agreement Meeting on Terminology and Definitions in Groin Pain in Athletes. During this consensus meeting GrP in athletes was classified into four major categories:3
First category: Adductor-related GrP in which adductor tenderness and pain on resisted adduction testing is present.
Second category: Iliopsoas-related GrP. This is more likely if there is pain on resisted hip flexion and/or pain on stretching the hip flexors.
Third category: Inguinal-related GrP. The pain is at the inguinal canal region level. No palpable inguinal hernia is present. The pain is aggravated with resistance testing of the abdominal muscles or during Valsalva.
Fourth category: Pubic-related GrP. The tenderness is at the pubic symphysis level and in the immediately adjacent bone.
The reality is that large terminological variations are still present in the contemporary literature. More recently Serner et al4 emphasised the need to standardise the terminology in order to facilitate the comparison of results from different studies. In this review the authors systematically reviewed 72 studies on GrP in athletes and found that 33 different conditions were referred to as ‘groin pain’. The lack of agreement concerning terminology can be explained, but not justified, by the fact that GrP symptoms can result from musculoskeletal, skeletal, gastrointestinal, urogenital, neurological and gynaecological problems.5 ,6
Groin Pain Syndrome Italian Consensus Conference background
The first Groin Pain Italian Consensus Conference was organised by Italian Society of Arthroscopy in Milan, on 5 February 2016, with the participation of 41 experts with different medical backgrounds: orthopaedics (16), sports physicians (3), general surgeons (7), physical medicine and rehabilitation physicians (5), physiotherapists (4), radiologists (2), sport physiologists (1) and physical trainers (3). Selection was based on Hirsch index, the number of publications concerning GrP and experience in the clinical evaluation, medical treatment and rehabilitation of GrP. Furthermore, the experts were not representing any organisations. All experts who participated to the Consensus Conference are the authors of this report.
Consensus Conference literature review process
Prior to the Consensus Conference two senior authors (GNB and PV) performed a literature review concerning the classification, clinical evaluation and imaging assessment of GrP. The review process was conducted as follows:
The research was performed independently by two authors, no language limitation was applied.
Databases used were MEDLINE, EMBASE, EXCERPTA MEDICA, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Review. The so-called ‘grey literature’ (ie, conferences, abstracts, thesis and unpublished reports) was not considered.
After a preliminary review of titles and abstracts of selected studies, the authors obtained full text of the studies which were most applicable to the three clinical issues mentioned above. Following review, all studies that did not report relevant information to these three specific clinical questions were excluded.
On the basis of the studies of major interest, the authors provided a comprehensive summary document divided into three distinct sections: diagnostic classification, clinical presentations, and imaging assessment. The document was delivered to each expert participating at the Consensus Conference, and was considered as a starting point for the discussion.
Consensus Conference presentation
The Consensus Conference experts aimed to approve three separate sections of the summary document:
Diagnostic classification document consensus;
Clinical presentations document consensus;
Imaging assessment document consensus.
During the discussion, each document was first presented by a facilitator (GNB), then followed by a plenary discussion guided by the chairman (PV), and then followed by a vote. The first document required 15 different discussions and same number of votes, while second and third document required six discussions and votes. During discussions the document was changed, and then voted again for the final version. The consensus was reached at the end of each discussion phase, where the majority of experts reached an agreement. In all cases, a unanimous conclusion was reached.
Summary of the first document: diagnostic classification document consensus
Unfortunately in the literature concerning GrP there is a lack of high-quality studies. In most studies the diagnostic criteria are, in the majority of cases, non-specific or incorrectly used in relationship to the pathologies.4 One of the major problems in this field is the lack of consensus on diagnostic criteria6 and taxonomy, making it impossible to decrease the heterogeneity between studies. Clear diagnostic classification would represent an important aid to improve the interpretation and the comparison of the different studies, thereby facilitating the decision-making process. For this reason the first Consensus Conference document was totally focused on taxonomy.
In this document the first vote concerned the use of the term groin pain syndrome (GrPS). The use of the term ‘syndrome’ is justified by the frequent overlapping of different clinical entities and by the possible cause–effect interaction that characterises a well-defined GrP clinic framework.7–9 Obviously, the term GrPS is an ‘umbrella term’ that must be complemented by the clinical framework description. You may then, for example, have a GrPS caused by adductor tendinopathy, inguinal hernia, or by a combination of pathologies. Only through adopting a comprehensive descriptive term such as GrPS, and associating it with the taxonomic description of the disease (or diseases) responsible for the symptomatology can we have a clear and rational classification of the problem. Consequently the following definition of GrPS was then proposed and approved:Any clinical symptom reported by the patient, located at the inguinal-pubic-adductor area, affecting sports activities and/or interfering with Activities of Daily Living (ADL), and requiring medical attention.
Furthermore in the same document (concerning the clinical classification) we propose that the aetiology of GrPS can be subdivided in 11 different categories, as follows:
Articular causes
Acetabular labrum tear
Femoroacetabular impingement (FAI) (I)
Hip antero-superior labral tear with avulsion of rectus femoris (HALTAR)
Hip osteoarthritis
Intra-articular loose bodies
Hip instability
Adhesive capsulitis
Legg-Calvé-Perthes disease and its outcomes
Dysplasia and its outcomes
Epiphysiolysis and its outcomes
Avascular necrosis of the femoral head
Sacroiliac joint disorders
Lumbar spine disorders
Synovitis
Notes: (I) CAM-FAI, pincer FAI, Subspine impingement (or anterior inferior iliac spine (AIIS) impingement).
Visceral causes
Inguinal hernia (I)
Other types of abdominal hernia
Intestinal diseases
Notes:
(I) Concerning inguinal hernia it is recommended to adopt the classification proposed by the European Hernia Society.10
Bone causes
Fractures and their outcomes
Stress fractures (I)
Avulsion fractures (II)
Iliac crest contusion (hip pointers) (III)
Notes:
Substantially concerning the pubic ramus or the femoral neck.
Mainly paediatric avulsion fractures involving the AIIS, the anterior superior iliac spine (ASIS), and the ischial tuberosity (ANIT).
Iliac crest contusions or hip pointers result from direct trauma at the level of iliac crest with subsequent formation of a periosteal haematoma. Such a haematoma can compress the lateral femoral cutaneous nerve and cause paraesthesia. 4. Musculotendinous causes
Rectus abdominis injuries
Rectus abdominis tendinopathy
Adductors muscles injuries
Adductor tendinopathy
Rectus abdominis—adductor longus common aponeurosis injuries
Iliopsoas injuries
Iliopsoas tendinopathy
Other indirect muscle injuries and their outcomes
Direct muscle injuries
Iliopsoas impingement (I)
Snapping internal hip
Snapping external hip
Bursitis (II)
Weakness of the inguinal canal posterior wall (III)
Notes:
Iliopsoas impingement with the medial portion of the acetabular rim.
Specifically concerning the iliopectineal bursa and greater trochanter seromucous bursa.
Indicated by: tenderness on palpation of the inguinal canal, tenderness on palpation at the level of the pubic tubercle and superficial inguinal ring dilation. In addition, in general manner, in case of conservative treatment failure the clinician must consider signs and symptoms that may suggest a serious disease.
5. Pubic symphysis related causes
Osteitis pubis
Symphysis instability (I)
Symphysis degenerative arthropathy
Notes:
(I) The radiological sign of symphyseal instability is represented by an asymmetry of pubic rami >2 mm visible in the Flamingo X-ray view.
Neurological causes (I)
Nerve entrapment syndrome (II)
Notes:
The category ‘neurological causes’ should be divided into two further subcategories. In the first category there is nerve injury due to overloading or overstretching (Neurological causes Category A). In the second category there is nerve injury due to an acute compression mechanism, or tear of the nerve (Neurological causes Category B).
Specifically concerning: lateral femoral cutaneous nerve; genitofemoral nerve (genital branch); ilioinguinal nerve; iliohypogastric nerve; femoral nerve; obturator nerve and pudendal nerve.
7. Developmental causes
Apophysitis (I)
Growth plate at pubic level (II)
Notes:
Specifically concerning the pubic ramus and less frequently the AIIS and ASIS.
Below 20 years of age it is common to observe anteromedial foci of endochondral ossification centres. These findings become particularly evident in MR arthrography.1
8. Genitourinary disease-related causes (inflammatory and non-inflammatory)
Prostatitis
Epididymitis
Corditis
Orchitis
Varicocele
Hydrocele
Urethritis
Other infections of the urinary tract
Cystitis
Ovarian cysts
Endometriosis
Ectopic pregnancy
Round ligament entrapment
Testicular/ovarian torsion
Ureteral lithiasis
9. Neoplastic causes
Testicular carcinoma
Osteoid osteoma
Other carcinomas
10. Infectious causes
Osteomyelitis
Septic arthritis
11. Systemic causes
Inguinal lymphadenopathy
Rheumatic diseases
After a deep examination and discussion concerning the literature, we proposed to subdivide the most common and probable diseases can cause GrPS in 11 different categories including 63 possible different clinical presentations (table 1).
The most likely causes of groin pain syndrome (GrPS) (63) grouped into 11 different categories
In the last part of the first approved Consensus Conference document a further subdivision of the GrPS in three main categories was proposed based both on the pathogenesis, and the onset of symptoms:
GrPS of traumatic origin, in which the onset of pain was due to any acute trauma, and this hypothesis is supported by medical history, clinical examination and imaging.
GrPS due to functional overload, characterised by insidious and progressive onset, without an acute trauma, or a situation to which the onset of pain symptoms can be attributed with certainty.
Long-standing GrPS (LSGrPS) or chronic GrPS, in which the cohort of symptoms reported by the patient continues for a long period (over 12 weeks) and is recalcitrant to any conservative therapy.
It is important to underline the fact that both functional overload GrPS and traumatic origin GrPS, may progress into LSGrPS. Similarly, a traumatic GrPS can occur in a previous framework of GrPS by overuse and/or LSGrPS. Finally, it is important to underline that LSGrPS is typically most commonly encountered in an amateur athlete, rather than in a professional one.11 ,12 A possible explanation is that an amateur athlete compared with a professional one does not have the same opportunities and access to preventative and suitable therapeutic procedures, either conservative or surgical. In any case we have to remember that LSGrPS is also frequently found in professional athletes due to their high level of training and play workload.
Therefore a correct definition of the diagnosis, corresponding to the concepts stated above, should include the following: ‘traumatic GrPS caused by…’, or ‘overuse GrPS caused by…’ or ‘LSGrPS caused by…’.
It is important to underline that, given the anatomical complexity of the pubic region, functional overload GrPS and LSGrPS can often be caused by overlapping clinical entities. In this case the diagnosis definition will change to: ‘traumatic or overuse GrPS, or LSGrPS caused by overlapping…’.
Furthermore it is important to note that it is useful to leave the classification open to other different diagnoses and an ‘idiopathic cause category’ represents an occurrence to consider.
Summary of the second document: clinical evaluation document consensus
Before describing the second document concerning clinical evaluation we would like to briefly describe the signs and symptoms of GrPS.
It is estimated that 5–18% of athletes seek medical care due to an activity-restricting GrPS.13–18 Within the same sport men had greater GrPS incidence than women with a risk ratio of 2.45.3 In effect, the proportion of GrPS is higher in men (12.8%) than in women (6.9%). In male club football GrPS accounted for 4–19% of all injuries, and only 2–14% in female club football.3 Symptoms are bilateral in 12% of the cases, it involves the adductor region in 40% of the cases, and the perineal region in 6% of the cases and for the remaining cases the inguinal zone. The pain onset occurs insidiously in 2/3 of the patients, and acutely in the remaining 1/3, while a certain number of patients report an acute event after a period of functional overload GrPS, or LSGrPS.15 ,19–24 The clinical presentation is characterised by spontaneous and evoked symptoms. Subjective symptoms are mainly represented by pain and functional deficits.25 ,26 From an objective point of view the patient may report of pain on palpation, during resisted muscle contraction, and during passive and active stretching. Clinical examination of the hip and its role in GrPS represents a challenge in clinical practice. To date we are seeing a growing interest concerning the hip labral pathology and FAI especially of CAM type. The CAM deformity (CAM comes from the Dutch word meaning ‘cog’) describes the femoral head and neck relationship as aspherical or not perfectly round. Unfortunately, at the moment there is no consensus on a gold standard for history and examination, and most tests show low diagnostic sensitivity and specificity.3 In any case the clinical examination must therefore be based on a series of tests focused on muscle contractions (isometric, concentric and eccentric), on the active and passive stretching manoeuvres27–31 and on palpation of some specific anatomical points.32–37
Thus based on both on the literature review13 ,16 ,26–29 ,31–35 ,37–50 and on present expert opinion, the second document was approved concerning clinical examination. The clinical examinations approved and recommended during the consensus were categorised as follows:
First category: specific test for adductor muscles
Palpation of the pubic insertion at common rectus abdominis/adductor longus aponeurosis.
Isometric squeeze test with proximal resistance (at knee level).
Isometric squeeze test with distal resistance (at ankles level).
Isometric squeeze test with distal resistance and abducted legs.
Isometric squeeze with flexed knee and proximal resistance.
Isometric squeeze test performed separately with the two legs with the use of a dynamometer (I).
Notes: (I) Optional test, but strongly recommended, especially in case of unilateral pain.
Second category: specific test for abdominal muscles
Palpation of the pubic insertion at common rectus abdominis/adductor longus
Rectus abdominis eccentric test
Sit-up pain test
Obliquus abdominis eccentric test
Third category: specific test for the hip joint
Hip joint intra and extra- rotation measurement
Flexion Abduction External Rotation (FABER) test
Flexion Adduction Internal Rotation (FADIR) test
Dynamic internal rotatory impingement test (DIRIT)
Dynamic external rotatory impingement test (DEXTRIT)
Posterior rim impingement test
Lateral rim impingement test
Fourth category: clinical evaluation of inguinal diseases
Palpation and clinical evaluation of the following anatomical structures:
Pubic tubercle
Pubic crest
Linea pectinea
Superior pubic ramus
Superficial inguinal ring
Inferior crus(inferolateral pillar or external pillar)
Superior crus (superomedial pillar or internal pillar)
It is important to note that the exact technical application of all proposed examination tests was also discussed, and during the discussion it has also emerged that the clinician, with respect to the investigated pathology, can also adopt other clinical tests at his/her own discretion.
Furthermore, as part of the second consensus document, the use of Copenhagen Hip And Groin Outcome Score (HAGOS) patient-reported outcome measures in its validated Italian form51 has been approved as a part of the medical history. The HAGOS questionnaire represents an important tool for the assessment of symptoms, activity limitations and participation-restrictions in physically active patients with GrPS. HAGOS is recommended as an important tool to assess the patient's quality of life in an objective manner.
Finally, there was consensus that an experienced multidisciplinary approach is important in the clinical evaluation of GrPS. Since GrPS can be caused by orthopaedic, visceral, and organic disorders and the fact that a rehabilitation programme is an important aspect of disease management, the involvement of orthopaedicians, surgeons, sport physicians, physiotherapists and physical trainers is vitally important.
Summary of the third document: imaging document consensus
The third document discussed and approved during the consensus involved imaging protocols. The protocols regarding conventional radiology (X-ray), ultrasound (US) examination, and MRI were discussed. No distinction was made between first-level and second-level examinations, because it was considered that each examination has a specific role. A correct imaging documentation is extremely important to help the clinical process. For this reason, these two aspects must be strongly correlated in order to avoid misinterpretation of radiological signs that are only incidental, and not related to the actual symptoms of the patient. The ideal situation is the development of a standard protocol that creates the greatest intraobserver and interobserver agreement, which are crucial factors in determining the reliability of radiological results. In any case, a well-defined imaging protocol is strongly recommended for all patients with GrPS.
Therefore based on the literature review1 ,16 ,52–73 and on expert opinion of the specialists present, the third document concerning the imaging assessment was approved, and is composed of the following routine examinations:
X-ray examination
The radiography routinely discussed and approved includes the following exams:
Anterior posterior view in upright position (AP1)
Anterior posterior view in upright position and alternately on one foot (Flamingo view) (AP2)
Dunn view (45° hip flexion view) (D)
From the radiographic assessment it is recommended to obtain the following information:
Presence of a cross sign (AP1) (overlap between the anterior and the posterior wall of the acetabulum)
Enlargement and/or erosion and/or sclerosis of the symphysis (AP1)
Symphysis asymmetry >2 mm (AP2)
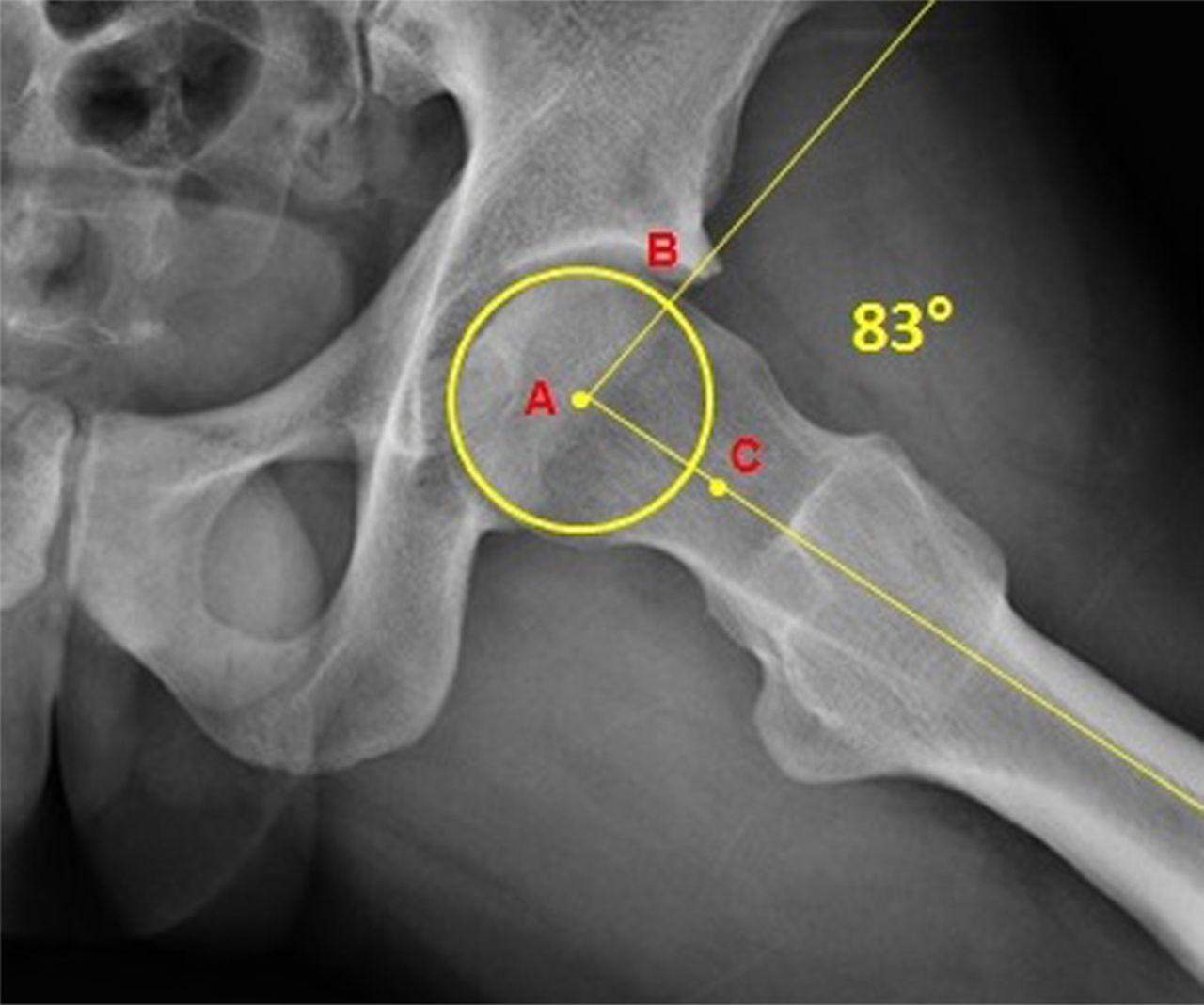
Calculation of α angle (D) (figure 1)
2 US examination.

Dunn view X-ray in which the α angle is calculated. The α angle is defined by the drawn best-fit circle (ie, the circle that best suits the sphericity of the femoral head) and identifying the point where the femoral head profile leaves this circle, a line is drown between the centre of this circle (A) and the identified point (B). A second line is drawn between the point A and the centre of femoral neck (C). The angle between these two lines is the α angle. An α angle measuring 55° or greater is considered a radiographic evidence of CAM-FAI (image from the private archive of Bisciotti GN).
US examination must provide the following assessments:
Assessment of the muscle tendon unit of the abdominal and adductor muscles.
Dynamic assessment of the inguinal canal structures.
Assessment of internal organs.
Assessment of the urinary tract and external genitalia.
US examination should be performed by a radiologist with specific expertise on GrPS imaging. Furthermore the presence of both a radiologist and a general surgeon is strongly recommended during the US examination. The presence of the surgeon during US examination is required in order to help rule out or confirm the diagnosis of inguinal or femoral hernia helping the radiologist both to identify the anatomical landmarks of the defect and the interpretation of the dynamic images. Furthermore direct and indirect hernia may be distinguished.74 ,75 The surgeon can also perform the examination of the superficial inguinal ring and canal under US guidance and emphasise the site of bulging.
MRI evaluation
Concerning the MRI evaluation, the use of a device of at least 1.5 T and a non-contrast protocol is recommended.
The recommended planes are:
Coronal
Sagittal
Axial
Axial oblique planes
Coronal oblique planes
Sagittal oblique planes
The acquisition sequences recommended are:
T1
T2 and T2 fat saturated (T2 FS)
STIR
Proton density fat saturation (PD FS)
The third document of consensus also suggests protocol for certain radiological findings:
The presence of bone marrow edema (BMO) at pubic symphysis level. The presence of BMO must be identified into the coronal STIR, coronal T1, axial oblique T2 FS, and PD FS sequences. Furthermore BMO should also be classified in I, II, or III degree, in relationship to its extension measured in the PD FS or T2 FS axial oblique plan sequences. BMO should be measured along the long axis of the pubic ramus. If BMO is extended <1 cm it is classified as I degree, if it is extended more than 1 cm but <2 cm it is II degree, finally if BMO is extended more than 3 cm is classified as III degree.53 ,56–58 ,65
Fatty infiltration within the BMO around the symphysis joint should be verified in the coronal STIR, coronal T1 and axial oblique T2 and PD FS sequences.66
Symphysis sclerosis should be assessed in coronal T1 and axial oblique T1 images.1 ,56–58
High-signal intensity parasymphyseal line should be verified in coronal STIR, axial oblique PD FS and sagittal STIR sequences.67 ,72 ,76
Secondary inferior and/or superior cleft sign should be assessed in coronal STIR, axial oblique PD FS and sagittal STIR sequences.55
Subchondral cysts/irregularities of the articular surface should be verified in coronal STIR and axial oblique images.1 ,56 ,57
Symphysis central disc protrusion should be estimated in coronal T1 and axial oblique T1 sequences.38 ,65
Adductor longus tendinopathy should be assessed in axial oblique sequences PD FS, T2 FS and T1, as well as in coronal T1 sequences.65–67 ,69
Adductor longus muscle–tendon injury should be evaluated in axial oblique sequences PD FS and T2 FS, as well as coronal STIR images.67 ,69 ,72 ,76
Rectus abdominis tendinopathy should be considered in sagittal STIR and axial oblique PD FS.54 ,55 ,66 ,72
Rectus abdominis muscle–tendon injury should be assessed in axial oblique plans PD FS and T2 FS, as well in coronal STIR.53 ,67 ,72 ,76
Growth plate at pubic symphysis level should be assessed in axial T1 sequences.66
The anatomical importance of the pre-aponeurotic fibrocartilaginous complex (PAFC) was discussed. The PAFC is formed by the interconnection of the tendons of the adductor muscles and the rectus abdominis muscle, and is a part of the parasymphyseal ligaments and the inguinal canal structures. It is important to understand that PAFC is in anatomical continuity with the central disc of pubic symphysis.76 This complex anatomical structure represents a real anchoring central point, and is therefore essentially formed by the interconnection of the fibres of the adductor muscles, rectus abdominis, external and internal oblique muscles, inguinal ligament, anterior pubic ligament, inferior pubic ligament, and fibrocartilage symphyseal disc. The acceptance of this anatomical concept leads to two fundamental points: the first one is the fact that the verification of anatomical integrity of PAFC is an important aspect of MRI examination and is crucial in reaching the diagnosis, while the second point is the necessity to consider the ‘anatomical continuity’ of the pubic symphysis, both its superficial and deep anatomical structures, as well as its functional continuity.
Guidelines
On the basis of the results of the Consensus Conference we propose the following guidelines in the GrPS clinical and imaging evaluation:
Step 1: Patient history completed by the HAGOS questionnaire. Both patient anamnesis and the compilation of HAGOS questionnaire must be made before clinical assessment. The anamnesis must be based on a thorough interview with the patient and a careful examination of his previous medical documentation.
Step 2: Clinical assessment mainly based on clinical tests proposed in the document 2 of the Consensus Conference (Clinical evaluation document consensus).
Step 3: Imaging evaluation. In GrPS due to functional overload and in LSGrPS it is strongly recommended to adopt the whole imaging routine examinations presented in the third document of the Consensus Conference (Imaging document consensus). In GrPS of traumatic origin the clinician/s may adopt a reduced imaging routine (in the flow chart, the possibility of choice among the various imaging tests is indicated with the dashed line).
Step 4: Formulation of the diagnosis based on the information collected in step 1, 2 and 3. If possible the diagnosis should be based on one, or more than one, of the 63 diseases listed in the document 1 of the Consensus Conference (Diagnostic classification document consensus).
Step 5: If the formulation of the diagnosis is impossible the patient may be advised for further diagnostic tests.
Step 6: Depending on the additional information obtained from step 5 (together with the information taken from the previous steps) the clinician(s) can make a diagnosis and advise the patient regarding the correct therapeutic procedure.
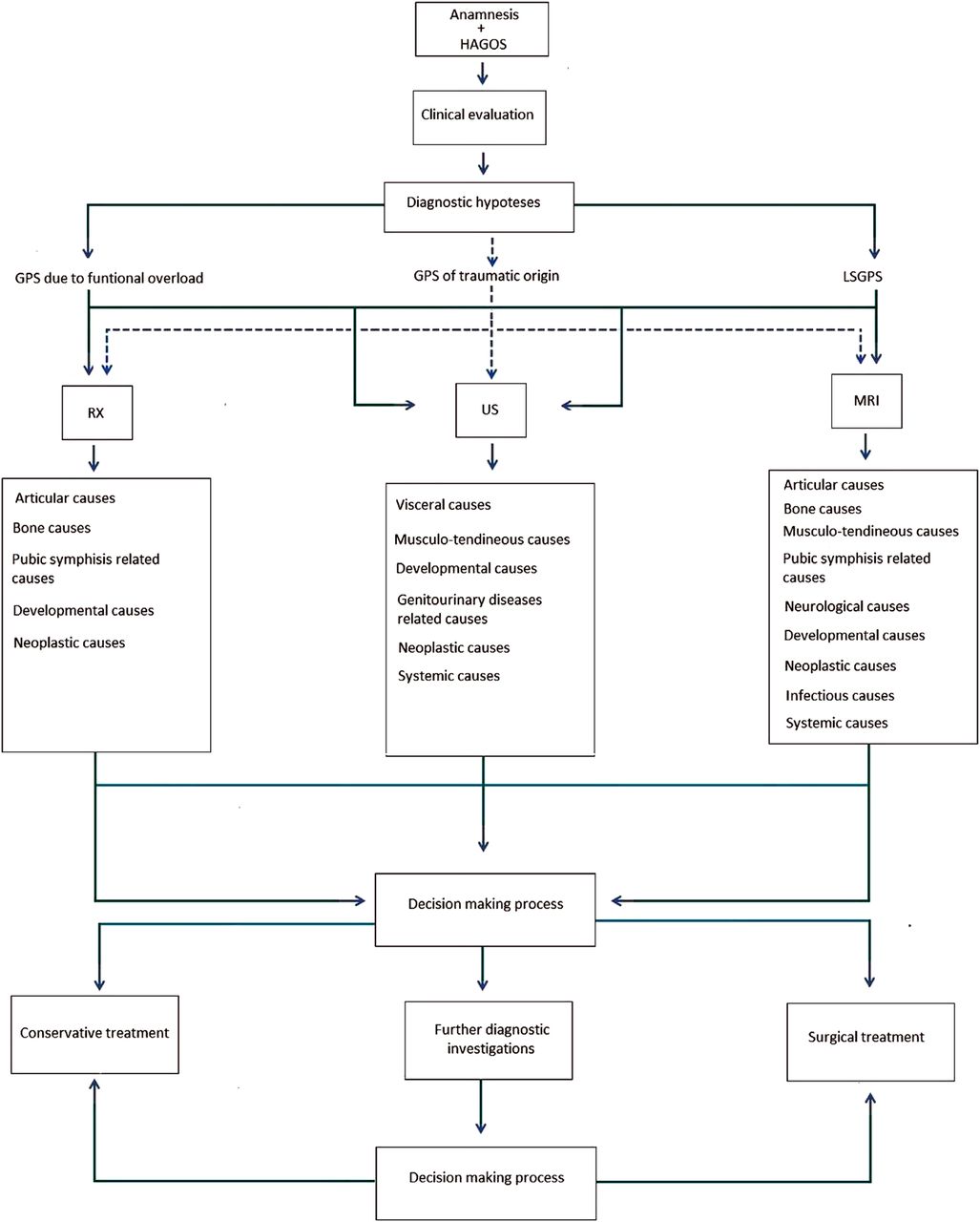
The above guidelines are shown in the flow chart represented in figure 2.
{kind=link}
{kind=link}
Flow chart based on the results of the Consensus Conference. After the anamnesis and the clinical evaluation the patient undergoes the imaging evaluation. The decision-making process is based on the results of clinical and imaging evaluations. In case of GrPS of traumatic origin (as explained in guidelines), the possibility of choice among the various imaging tests is indicated in the flow chart with the dashed line. In the case in which it is possible to have a diagnosis the patient may be advised for a conservative or surgical treatment. In the case in which a diagnosis is not reached the patient may be advised for further diagnostic investigations (ie, blood tests, urine test, CT, scintigraphy etc) in order to obtain diagnosis and decide the treatment pathway. GrPS, groin pain syndrome; HAGOS, Copenhagen Hip And Groin Outcome Score; LSGrPS, long-standing GrPS; RX, radiography; US, ultrasound.
Conference Consensus conclusions
The main strength of the GrPS Italian Consensus Conference was the presence of recognised leading experts in this field with different backgrounds. This multidisciplinary study guaranteed a thorough and comprehensive approach to the topic.
Some important points of discussion and reflections emerged from the Consensus Conference, and can be summarised as follows.
The controversy regarding the GrPS nomenclature can only be solved through the adoption of a common language, which would satisfy the principles of clarity, fairness and sharing.
The adoption of guidelines, both from a clinical and imaging point of view, is a first step towards harmonising and rationalising the approach to GrPS. Obviously, such guidelines do not limit the clinicians' professional skills, but are rather a guide that facilitate reaching a definitive diagnosis, enabling this to be based on well-defined clinical diagnostic steps. Furthermore the use of HAGOS questionnaire provides the ability to objectively quantify the therapeutic effectiveness of proposed procedures. Finally, an experienced multidisciplinary approach in the clinical evaluation of GrPS, and especially in LSGrPS is strongly recommended.
A standardised imaging protocol would facilitate the comparison of data from different study groups, and substantially favour the logical-deductive process that is the basis of the diagnostic pathway. In any case, further and more detailed studies are needed to clarify the true significance of some radiological findings that we can observe in a GrPS framework.
Future directions
The weak point of this Consensus Conference was the paucity and lack of high-quality studies present in the literature. This represented a problem concerning scientific support to substantiate and validate the experts' various opinions. For this reason the conclusions of this Consensus Conference do not represent evidence, but rather guidelines.
The relatively small number of female participants in the present literature could theoretically be a limitation for the applicability of the data described above to a female population. Further studies focused on female population are needed.
Finally, we would like to point out the need for future multidisciplinary Consensus Conferences that could help to further clarify this difficult field of study.
References
Footnotes
Contributors GNB, PV, RZ, AAu, GC, FDM and ZV planned the manuscript. All authors contributed to the writing and editing of the manuscript and gave their approval for its final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.