Article Text

Abstract
Background This article addresses typical injury patterns related to the traditional Swiss team sport of Hornussen. A small plastic disk is struck with a special elastic racket and then intercepted in the field. Severe injuries have occasionally been reported. We present a systematic review of all cases of Hornussen injuries treated in the University Hospital of Bern from 2000 to 2014.
Methods To assess the frequency, type and outcome of Hornussen injuries, we performed a database search of all inpatient and outpatient cases related to Hornussen and that were admitted to and/or treated in Bern University Hospital from 2000 to 2014.
Results A total of 28 such patients could be identified. Apart from 1 woman injured as a bystander and treated as an outpatient, all patients were male and active players. Typical injury patterns comprised midfacial fractures and severe ocular traumata, very often in combination. Almost all of these patients had to be hospitalised due to the severity of the trauma suffered and underwent surgery. 1 patient had to be admitted to the intensive care unit prior to the operation.
Conclusions Eye and face injuries caused by Hornussen can be devastating. This resembles the potential risk of other bat-and-ball sports, such as cricket and baseball. Apart from the economic loss due to treatment costs and sick leave, these injuries can be disabling for life. It should therefore be mandatory for all players to wear protective gear, as is already the case for Hornussen players born in 1984 or later.
- Eye
- Facial bones
- Sporting injuries
- Trauma
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
This is the first in-depth assessment of characteristic Hornussen sport injury cases admitted to a level I trauma centre in Switzerland.
Midfacial fractures combined with blunt or perforating ocular traumata were found to be frequent injury patterns.
Injuries were mostly severe and the majority of patients had to be hospitalised and surgically treated.
An effective precaution would be helmet protection for all Hornussen players.
Introduction
Hornussen is an indigenous national team sport originating in the Central Swiss Plateau. A small plastic disk (the ‘Nouss’ or ‘Hornuss’) is placed on a launching ramp (the ‘Bock’) and struck with a small block made of compressed hardwood (the ‘Träf’), which is fixed at the end of a special elastic racket (the ‘Stecken’) by a member of one team (figure 1) and then intercepted (‘abgetan’) in the field (‘Ries’) with special wooden shields (the ‘Schindeln’) by members of the other team (figure 2).1–3 During the match, both teams play both parts of the game. The team with the better intercepting performance wins the match. If the interception results are identical, the team with the greater total flight distances of the Nouss wins. Thus, in Hornussen, ‘defence’ is more important than ‘attack’.

Hornussen player driving the Nouss off the Bock. (Inlay: Träf at the end of the Stecken approaching the Nouss).

Hornussen players intercepting the Nouss (upper left corner) in the Ries with their Schindeln.
The exact roots of Hornussen are unknown. It may have emerged from the heathen custom of hitting burning logs from the mountain to the valley to cast out demons4 or perhaps from medieval war games.5 Hornussen was officially documented for the first time in 1625, when four men were reprimanded by the consistory of Lauperswil for playing Hornussen during ‘catechisation and prayer service’.6 7 Interestingly, the first Hornussen accident was reported as early as 1738, after a player had been fatally wounded to his carotid artery by a broken Stecken.6 ,7
The rules of the game have progressively evolved since the 17th century. Today Hornussen is performed with standardised and highly developed equipment (eg, high-tech Steckens made of carbon fibre), as an organised team sport with championships in different leagues under the aegis of the national Swiss Hornusser Association (Eidgenössischer Hornusserverband)8 with currently 7411 licensed members (Eidgenössischer Hornusserverband, personal communication). Up to 80% of these fall within the scope of our hospital's catchment area (Eidgenössischer Hornusserverband, personal communication).9 The number of unorganised casual players is unknown.
The Nouss itself weighs 78 g and is 62×32 mm. It is placed and fixed on the Bock with a small piece of clay (figure 1). When struck with the Stecken's Träf, the Nouss reaches initial velocities of 80–85 m/s (ie, around 300 km/hour), with an initial energy of about 250 J.5 ,10 After a flight of ∼300 m, the impact energy of the Nouss is still about 60–70 J, resulting in energy density values between 0.15 and 0.3 J/mm² when hitting soft or hard tissue (eg, skin or bones). This is more than sufficient to cause contused lacerations or fractures of thinner bones, for example, those in the midface.5 ,11
These hazards resemble those in better known bat-and-ball sports like cricket or baseball. However, Hornussen is mostly performed without any protective measures such as helmets. Apart from the aforementioned historic reference of 1738, severe injuries have been reported in two scientific publications12 ,13 and occasionally in the daily press,14–16 especially devastating ocular injuries. These injuries can be avoided by wearing protective equipment, depending on the type of injury.
Bearing this in mind, we retrospectively evaluated the type and severity of the injuries caused by this sport. To the best of our knowledge, there has been no systematic review of Hornussen accidents before. This is therefore the first in-depth study of injuries and injury patterns caused by Hornussen.
Methods
Hospital unit and patient population
The University Department of Emergency Medicine of the Inselspital Bern serves as a level I centre for patients older than 16 years, and commands a catchment area of 1.5 million people. It treats more than 38 000 patients each year.
Our study was performed as a retrospective database query of all patients admitted to or initially treated in the Emergency Department from 1 January 2000 to 31 December 2014. The software used was Qualicare17 (Qualidoc AG, Trimbach, Switzerland) and E.Care (E.Care BVBA, Turnhout, Belgium). Case files related to Hornussen were identified by corresponding search terms and exported anonymously. Restriction to active players was not intended.
The database entries comprise basic demographic data (eg, age and gender), as well as relevant historical details of medical symptoms or the type of accident (eg, direct or ricocheted hits by a Hornuss or hits by the Stecken). The database also provided the results of clinical consultations and radiological examinations, together with medical and traumatological diagnoses and information on treatment after admission. The short-term outcome was defined by the type of care given to each patient (outpatient, inpatient, intensive care unit (ICU), surgery or no surgery) and recorded as well.
Application of the FISS
In so far as was retrospectively possible, we also classified the patients by means of the Facial Injury Severity Scale (FISS; table 1). FISS was introduced in 2006, primarily as a tool for the assessment and management of maxillofacial trauma.18 ,19 It was subsequently adopted for research and has become the most frequently cited tool for scoring maxillofacial trauma.20 FISS yields a numerical value composed of the sum of individual fractures and/or fracture patterns. It ranges from 0 to over 25 in theory, but the highest FISS reported in the initial publication with 1115 patients was 13.18
Facial Injury Severity Scale (FISS)
Our database entries proved to be complete enough to allow reliable determination of each patient's FISS. The exact extent of facial lacerations was not recorded in all cases, but never came close to a combined length of 10 cm. Consequently, we decided always to assign 0 points for this item, although it remains possible that the FISS of a very few patients was then under-rated by 1 point.
Data were fully anonymised before analysis and therefore, according to local law, no prior consent was necessary. Statistical evaluation was purely descriptive, due to the small sample size.
Results
Sample size
A total of 39 case files from the period 1 January 2000 to 31 December 2014 were initially identified as being related to Hornussen accidents. After rigorous inspection of each file, 11 patients were excluded from further analysis as they were found not to be specifically related to Hornussen accidents. Typical examples comprised acute cardiological or neurological episodes suffered during Hornussen like coronary ischaemia or stroke, as well as falls or stumbles leading to a torn muscle fibre or a broken ankle.
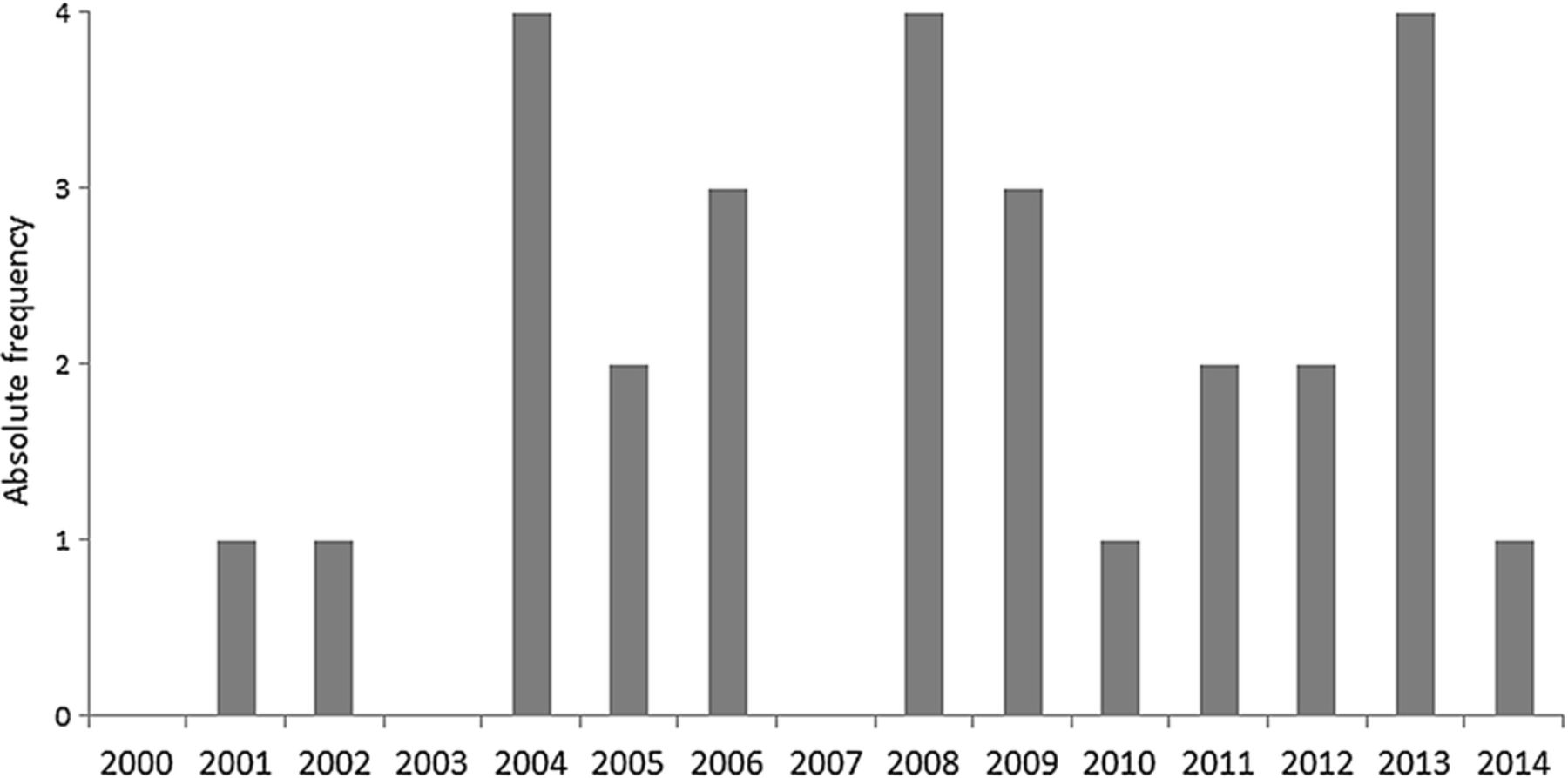
The remaining 28 case files showed a more or less constant annual rate of 0–4 Hornussen accidents admitted to the University Emergency Department each year (figure 3). There was only one female patient (4%), who was involved as a bystander; 27 patients (96%) were active male players aged between 19 and 71 years (median 40.4 years). Although this female patient did not represent the typical risk group, she was kept for data evaluation as the trauma mechanism was definitely characteristic. It was striking that none of these patients had used any protective gear.

Annual distribution of admissions for Hornussen accidents between 2000 and 2014.
Typical injuries and treatment
The face and skull (n=26) were the most frequently injured body regions (93%, figure 4). The remaining patients (n=2) suffered injuries to the upper and lower extremities (7%). These two patients were treated as outpatients, one after minor surgery under local anaesthesia. Twenty-two (79%) of the patients were hit by a flying Nouss, 4 (14%) were injured when striking the Nouss, either by hitting themselves with the Träf or by being hit by parts of a broken Stecken or Nouss. For two patients (7%), no clear description of the accident's circumstances was found in the case file.

Distribution of injured body regions.
As the vast majority of 26 patients suffered injuries to the face and skull only, many with complex trauma patterns, we concentrated on the extensive analysis of these cases. The detailed information for each patient can be found in table 2.
Patients' characteristics
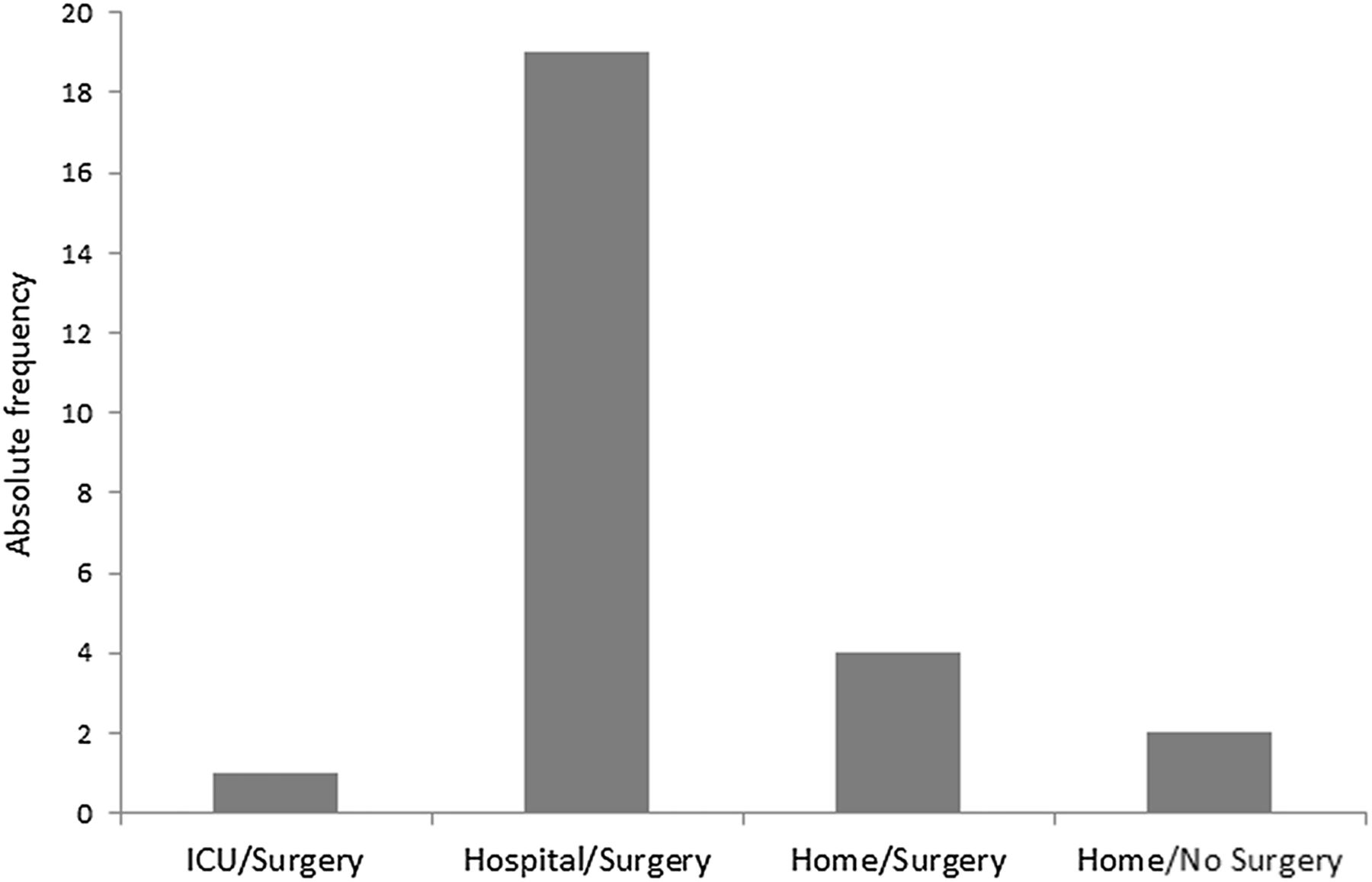
As aforementioned, the impact energy of the Nouss when reaching the Ries is easily above the limit for causing severe damage to soft and hard tissues. Thus, it was no surprise that 20 of 26 patients (77%) with face/skull injuries had to be hospitalised due to the severity of the trauma and that all of those patients had to undergo surgery. One patient with subdural haematoma was admitted to the ICU for monitoring prior to operation (figure 5).

Patient outcome. ICU, intensive care unit.
Six patients (23%) could be treated as outpatients; four underwent minor surgery such as wound cleaning and suture. The median outpatient FISS was only 0.5 (SD 0.83, maximum 2); in contrast, the median inpatient FISS was 1.9 (SD 1.68, maximum 7).
The most common injuries found were soft tissue lesions (92%)—predominantly (19 out of 24 cases) contused lacerations—and fractures (69%), mainly of the midface and the orbital cavities. Significant ocular trauma (blunt and perforating) was found in 35% of our patients. There were two patients with tooth damage (8%). A total of 54 injuries were recorded in 26 patients (figure 6), most patients suffered combined trauma.

Type of injuries.
Combined trauma as a rule
The most frequent combination was fracture and contused laceration, in 15 of 26 patients (58%). Seven out of 9 (78%) patients with significant ocular trauma also exhibited at least one fracture and one contused laceration (figure 7). The remaining two patients were affected by an ocular trauma combined with a fracture and a superficial haematoma or by an isolated perforating ocular trauma caused by a shattered eyeglass lens.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
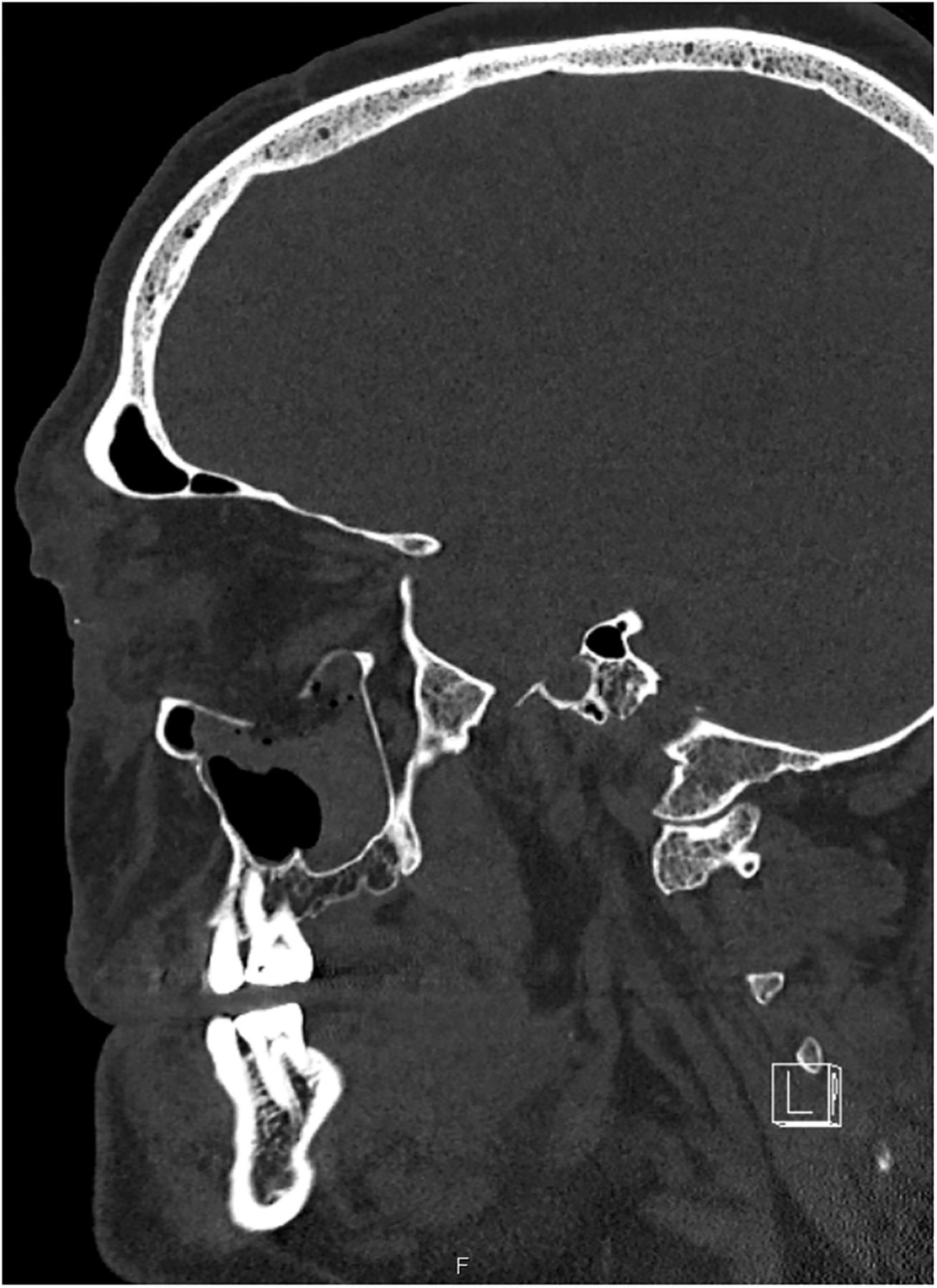
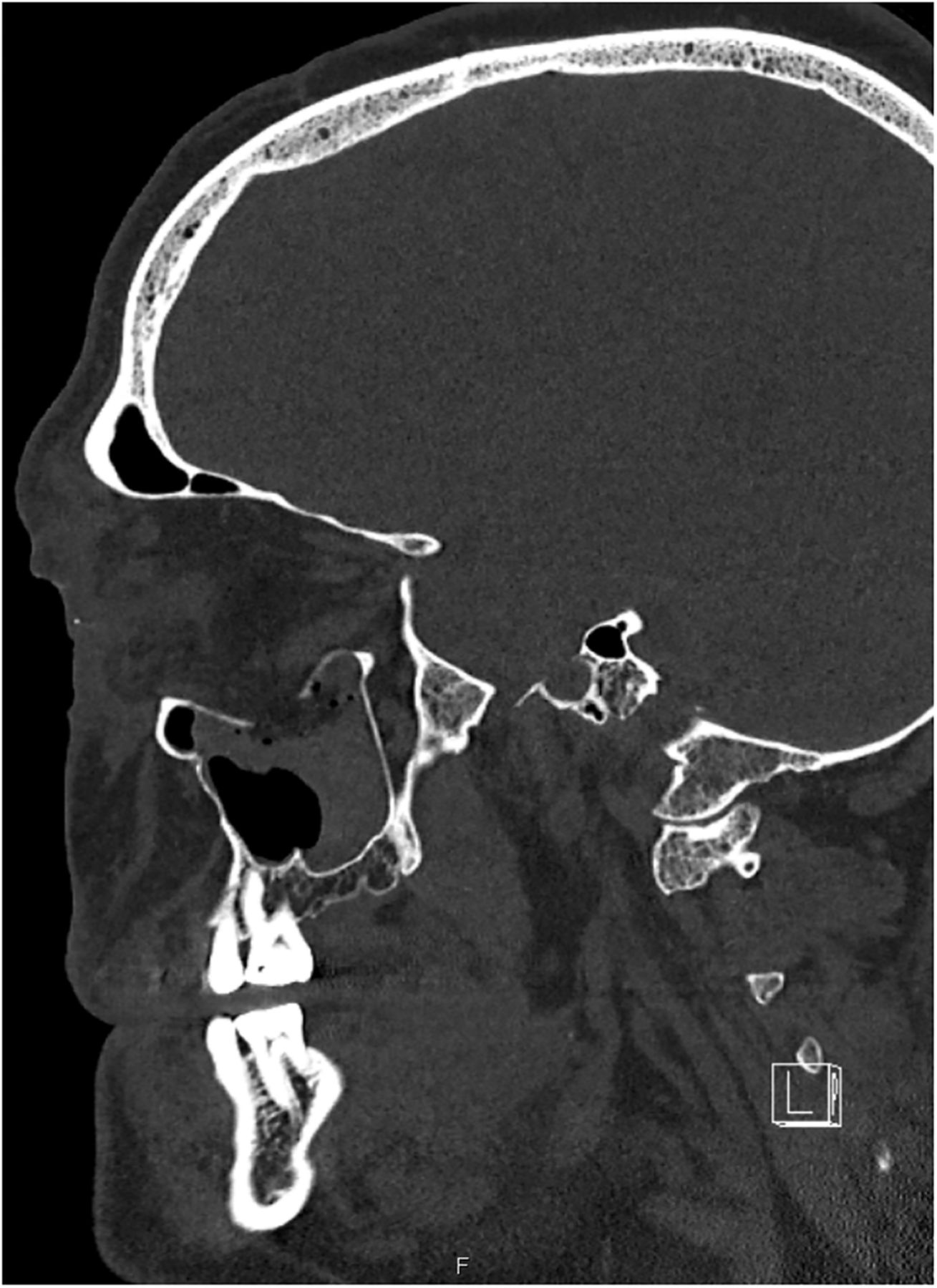
Sagittal CT scan of the midface demonstrating an extended orbital floor fracture caused by a Nouss. This patient also suffered significant ocular trauma.
There was a clear trend that the outcome of patients depended on the complexity of the injuries. Of the eight patients with a single injury, four could be treated as outpatients and four were admitted to hospital care. Seven of nine patients (78%) with two different injuries had to be hospitalised, as were all patients with three different injuries. The only patient with four different injuries was admitted to the ICU. These last two groups had all suffered from severe ocular trauma or subdural haematoma.
Interestingly, there was essentially no difference between the patients hit by a ricocheted Nouss (n=5) and the others (n=15, 2 direct hits and 13 cases without detailed information). Apart from the one female patient, who was most probably hit by a Nouss that was already moving slowly, three of the four active players suffered severe midfacial trauma, as well as one with additional severe blunt ocular trauma. The mean FISS caused by ricocheted hits was 1.4 vs 1.87 (direct hits or unclear).
Discussion
The typical patient affected by a Hornussen accident is an active male player with a mean age of about 40 years who did not use protective gear. Although in 1999 the Swiss Hornusser Association made protective helmets with face shield (either cage or polycarbonate visor, similar to ice hockey equipment) mandatory for players born 1984 or after, we found two younger patients (born in 1988 and 1986) with midfacial trauma (FISS 1 in both cases); one of them additionally suffered from a severe blunt ocular trauma. Neither of these patients had used a helmet.
Ophthalmological injuries
Ocular trauma caused by Hornussen generally tends to be severe.12–16 This was confirmed by our nine such patients, whose blunt and perforating/penetrating ocular injuries required surgical intervention in all cases. Typical clinical findings comprised corneal laceration and perforation, iridal trauma and lens dislocation. Unfortunately, our data can give no information about early complications or secondary surgery (eg, enucleation). This is also the case for long-term sequelae, such as glaucoma, impaired visual acuity or even blindness. However, the medical literature provides evidence that significant visual impairment is a regular consequence of Hornussen or other similar sports accidents. Caduff12 mentioned six patients with severe ocular damage after Hornussen, which led to the payment of pension funds in four of these cases. Casotti et al13 described a small series of three Hornussen players with ocular injury after one direct and two ricocheted hits by a Nouss, which caused one perforating and two blunt contusional ocular lesions. The perforation injury led to blindness; moreover two patients suffered orbital roof and floor fractures. Similar cases have been reported in the daily press.14–16 Weitgasser et al21 reviewed seven cases of ocular trauma from golf and mentioned the additional risk of perforated globes from shattered eyeglass lenses. This was precisely the case in two of our patients. Other publications have reported comparable serious eye injuries from other sports or recreational activities, such as paintball,22 badminton and ice hockey.23 Approximately 30–40% of the cases resulted in permanent and significant visual impairment or even legal blindness. Seventy-two per cent of all sport-related eye injuries may have to be followed up for life, as they are accompanied by an increased risk of glaucoma.23 The outcome is even worse for perforating and penetrating eye injuries requiring open globe repair. Depending on trauma severity and infectious complications (endophthalmitis), ∼70% of these patients may suffer blindness and up to 29% enucleation.24 ,25 It is clear that the characteristics of Hornussen-induced eye injuries cannot so easily be compared with those inflicted during other sports, as it must be emphasised that a Nouss significantly exceeds the size of a golf ball, or a shuttlecock in badminton. Thus, these projectiles fit better into the orbital cavity than a Nouss does and more easily cause eye injury. The Nouss, however, consistently leads to fractures of the bony structures of the orbita and other midfacial bones that protect the eye, as it is harder and larger. But after the accident, the severity and outcome of Hornussen eye injuries may not essentially differ from other types of eye injury.
Maxillofacial trauma
There is much less recent literature on sport-related midfacial/maxillofacial fractures than on sport-related eye injuries. Perhaps the potential loss of a sensory organ encourages more research and publication than reports of ‘simple’ fractures. Moreover, there are notable cultural influences, as many studies originate from central Europe and deal with the favourite local sports, mainly soccer, which predominantly leads to mandibular fractures.17 ,26 ,27 Bat-and-ball sports like baseball or cricket typically cause maxillofacial fractures and are more or less restricted to Anglo-American and Australasian publications.28–33 But in general, all authors found that the typical patient affected by such fractures is a male, with a gender ratio mainly around 7:1 to 14:1 (maximum 36:1).26–33 This fits well to our own patient group and is of course because more or less all of the evaluated sports are mostly performed by male participants. Studies focusing on facial trauma resulting from activities of daily life have found a much more balanced gender ratio of around 2:1.34 ,35 Papers on cricket or baseball consistently report midfacial/maxillofacial fractures. Injuries to the orbitozygomatic region are most typical, and impact from a ball is the most frequent cause.28–33 This is also totally consistent with our present results. On the other hand, the age distribution of our Hornussen sample differs from that in other sports, as soccer, rugby and baseball are predominantly played by participants below 35 years of age, whereas 8 of our 28 patients were aged 50 years or more.
But to what extent do maxillofacial fractures compromise post-traumatic well-being compared with ocular injuries? Transient and persistent post-traumatic damage of the sensory infraorbital nerve was recorded most frequently (up to 66%) and is a consequence of orbitozygomatic fractures.36–38 Sustained damaged motor function of the facial nerve would definitely have a greater impact on the individual than a damaged pure sensory nerve and was reported with a frequency of 2.3%.38 Functional ophthalmological impairment from persistent diplopia, enophthalmos or limited eye movement was an additional complication in ∼15% of patients.36 ,38 Chronic rhinosinusitis with facial pain and disturbed sleep have also been described after surgical intervention in midfacial fractures.39 Could these findings be representative of our study population as well? The median FISS of our 16 patients with midfacial fractures (excluding the two patients with isolated mandibular fracture) was 2.25. The median FISS values of larger groups of patients covered a range from 1.37 to 1.97.37 ,40 Only patients injured by traffic accidents or falls from heights above 3 m displayed considerably higher median FISS values of 3.4–6.0.20 ,40 ,41 Thus, we conclude that our Hornussen injury patients reach midfacial trauma levels comparable to those of other populations—except for serious traffic accidents and falls—and may be equally affected by the long-term complications of maxillofacial fractures.
Conclusions and suggestions for prevention
Most Hornussen accidents do not of course involve severe midfacial or ocular trauma. Fractures of the fingers or contusions/contused lacerations of the trunk or the extremities, as found in two of our patient sample, are certainly much more common Hornussen injuries.15 ,16 These minor injuries are very seldom admitted to a university level I trauma centre but are regularly and adequately treated in smaller communal or regional hospitals of, for example, level III. Consequently our data are affected by a marked selection bias. We made an informal inquiry to the Swiss National Accident Insurance Fund (SUVA, Schweizerische Unfallversicherungsanstalt) and were informed that around 100 Hornussen accidents yearly are reported and dealt with by the leading accident insurer of Switzerland. This would suggest that the frequency of significant maxillofacial or ophthalmological trauma can hardly be higher than 2% or 3% of all Hornussen incidents, as we surveyed 26 cases within a time frame of 15 years and our university hospital's catchment area reaches ∼80% of all organised Hornussen players (Eidgenössischer Hornusserverband, personal communication).9 But apart from the individual consequences of these rare catastrophic events, which can change a life forever, major trauma entails a high economic burden on the community, through treatment costs and sick leave. It is well documented for other sports that compulsory wearing of protective gear greatly reduces severe head injury.42–45 Consistent use of protective helmets with additional face shield should therefore be made mandatory for all age groups of Hornussen players and preferably not be restricted to the intercepting players in the field, as 4 (15%, median FISS 1) of our 26 patients were injured while punting the Nouss from the Bock. The existing regulation for players born 1984 or after should accordingly be expanded.
Acknowledgments
The authors thank Sebastian Wolf, Department of Ophthalmology, University Hospital Bern, for reviewing this article.
References
Footnotes
Contributors AE motivated the planning and the conduct of the study. MR provided the clinical database research. VW drafted the manuscript and performed the statistical evaluation. BS helped to transform the clinical data into the Facial Injury Severity Scale (FISS) score values. All authors gave editorial input, read and approved the final revision of the submitted manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.