Article Text

Abstract
Objective The objective of this study was to provide an update of the evidence on the efficacy of gross motor development interventions in young children (0–5 years) from 2007 to 2015.
Methods Searches were conducted of six electronic databases: PUBMED, Medline (Ovid), ERIC (Ebsco), Embase, SCOPUS and Psychinfo. Studies included any childcare-based, preschool-based, home-based, or community-based intervention targeting the development of gross motor skills including statistical analysis of gross motor skill competence. Data were extracted on design, participants, intervention components, methodological quality and efficacy.
Results Seven articles were included and all were delivered in early childhood settings. Four studies had high methodological quality. Most studies used trained staff members/educators to deliver the intervention (86%) and five studies lasted 18 weeks or more. Six studies reported statistically significant intervention effects.
Conclusions Despite the proven importance of gross motor skill development in young children and the recommendations made in the previous review, this review highlights the limited studies evaluated to improve such key life skills in young children over the past 8 years.
Trial registration number CRD42015015826.
- Children
- Children and exercise
- Physical activity
- Review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings
The quality of the intervention studies has improved, but not the quantity since only seven studies have examined gross motor skill interventions in young children (>5 years) over the past 8 years.
Professional development of the educators in the area of gross motor skills development should be an important component in future interventions to increase the quality of their practice in early childhood settings.
Parent involvement in interventions is recommended given their important role in developing gross motor skills through role modelling and providing opportunities, encouragement and support.
Introduction
Fundamental or gross motor skills (GMS) are the foundation for many sports and physical activities. From a health perspective, higher levels of GMS are associated with lower body mass index1 better cardiorespiratory fitness2 and physical activity3 as well as enhanced cognitive development4 ,5 social development and language skills.6 Moreover, children with poor GMS are more likely to have lower self-esteem7 ,8 and higher levels of anxiety.9
GMS proficiency in young children is suboptimal10 ,11 and given the short-term and long-term consequences of poor skills, interventions targeting the improvement of these skills are needed. In 2009, Riethmuller et al12 conducted a systematic review, which assessed the efficacy of interventions designed to increase GMS in young children (<5 years). Seventeen articles were included, of which most were controlled trials (65%) and implemented in early childhood settings (65%). More than half of the studies reported statistically significant improvements (60%). The review highlighted the limited quantity and quality of interventions in young children and the lack of high-quality evidence in this area.
In recent years, several studies have reported on the relationship between GMS and other important developmental areas adding evidence to the importance of GMS development. Jenni et al13 found positive correlations between motor and intellectual functions, and Leonard and Hill6 highlighted the significant relationship with the development of social skills and language. As this is an area of interest internationally, there is a need for a further review which updates the evidence in this area and gives directions for further research to promote GMS development. The aim of the current review was to provide an update of the evidence on the efficacy of gross motor development interventions in young children (0–5 years) and to provide recommendations for further research in this area.
Methods
This review followed the guidelines in the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement.14
Eligibility criteria
Types of participants
Children between the ages of 0 and 5 years (mean age >5 years) enrolled in kindergarten, childcare centres, preschool or community services, but not yet at school.
Types of intervention
Any childcare-based, preschool-based, home-based or community-based intervention targeting the development of GMS. Targeted skills could include locomotor and object control skills.
Types of outcome measures
Studies were included if they reported statistical analysis of GMS competence with measurements taken pre- and at least once postintervention and included either process (knowledge of performance) or product (knowledge of results) assessments of at least one skill.
Types of studies
Randomised controlled trials (RCTs) with experimental and quasi-experimental designs and single group pretest and post-test designs. Studies were excluded if they: (1) targeted groups from special populations (eg, children with cerebral palsy or autism); (2) no full text was available; (3) the research was not published in English.
Information sources and search
Six electronic databases were searched: PUBMED, Medline (Ovid), ERIC (Ebsco), Embase, SCOPUS and Psychinfo with a restriction on the start of the publication date to 2007 and before given the previous systematic review.12 The search was performed in January 2015. The following search terms were used: toddler OR childcare OR day care OR preschool* OR ‘early childhood’ OR ‘community-based’ AND random* OR trial OR evaluation OR programme OR pilot AND ‘motor skill*’ OR ‘movement skill*’ OR ‘motor development’. Additional studies were found through scanning reference lists of included articles.
Study selection
After searching the databases, one of the authors (SLV) removed all duplicates and two authors (RAJ/SLV) screened all titles and abstracts in a non-blinded standardised way. These were screened for inclusion, by dividing them into three groups: ‘yes, no, or maybe’. All decisions were checked by another author (ADO) and a discussion followed when there were any disagreements. The full text for the remaining articles was retrieved.
Data collection process
After the study selection process, one author (SLV) extracted data on methodology, characteristics of participants, interventions programme, GMS measurement and results from the selected studies. These data were checked by another author (RAJ).
Methodological quality
Methodological Quality was assessed by using a 10-item quality assessment scale (see table 1) adapted from previously used methodological assessments.15 ,16 Each included article was assessed by two authors (ADO/SLV) individually. Any disagreements between the authors were resolved by discussion. An article was classified as high methodological quality when it scored ≥5 for a controlled trial and ≥6 for a randomised controlled trial.16
Methodological quality assessment items15
Synthesis of results
The following data were extracted from the articles: research design and setting, sample size and mean age, total duration of the intervention in weeks, intervention groups, intervention content, measurement of motor skills and results.
Results
Overview of studies
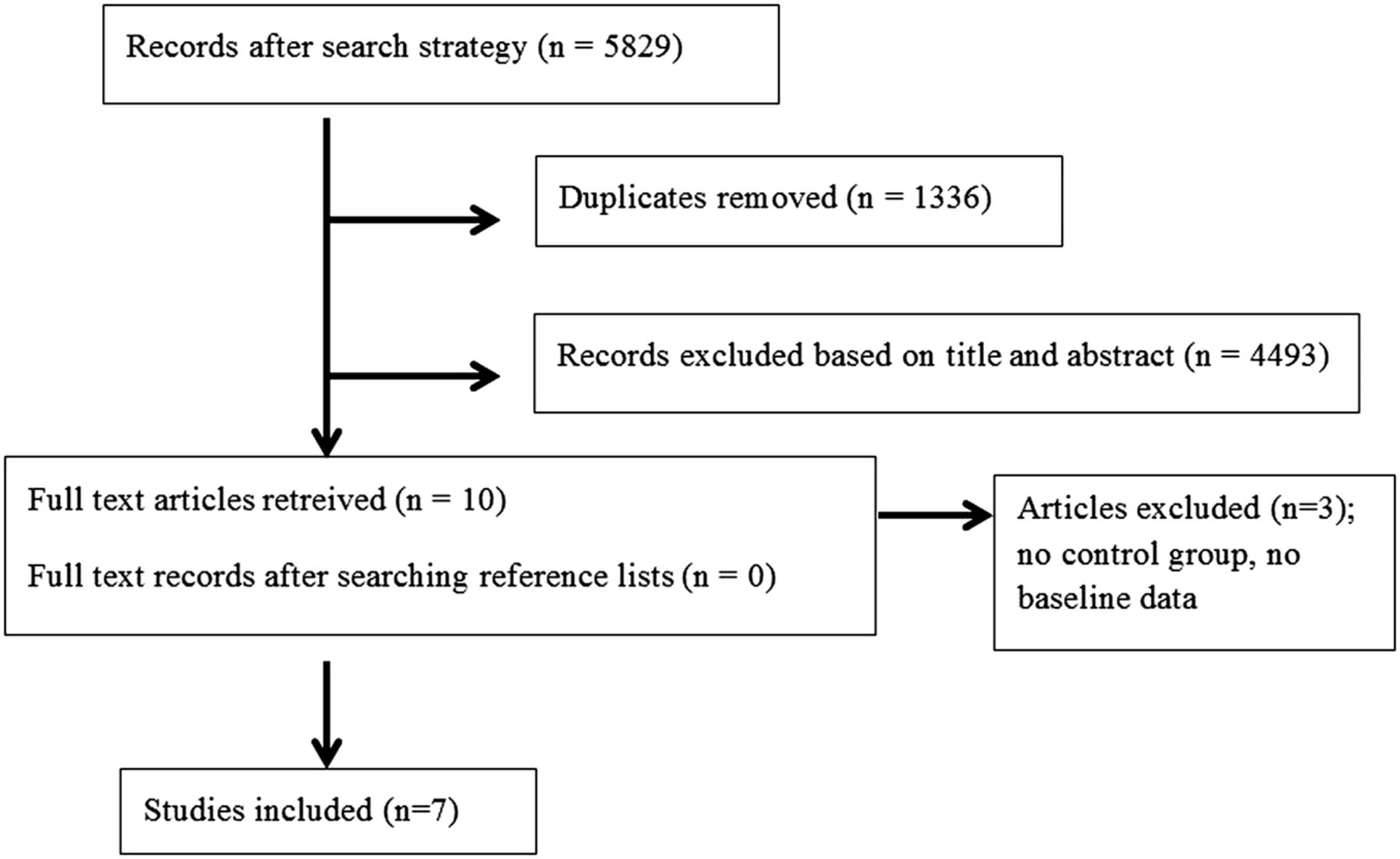
Study selection is displayed in figure 1. The initial search identified 5829 hits. After removing duplicates (n=1336) and screening of titles and abstracts (n=4493), 10 articles remained. The full-texts of these articles were retrieved and seven articles were included.

{kind=link}
PRISMA flowchart of studies through the review process.
Study characteristics
Table 2 shows characteristics of the studies. Five studies were published between 2011 and 2014.17–21 Three studies were conducted in the USA17 ,18 ,22 two studies were conducted in Australia20 ,23 and the others were conducted in Switzerland19 and Greece.21 Some studies recruited centres based on region19 ,21 or within an existing program17 while others worked together with the (local) government23 or childcare organisations.18 ,20 ,22 Two studies involved parents.
Description of study characteristics
There were six randomised controlled trials17–19 ,20 ,22 ,23 and one quasi-experimental study.21 The sample size of the studies varied from 7117 to 835 participants.19
Implementation
All interventions took place in early childhood settings and most were delivered by setting staff.17–19 ,20 ,23 Professional development sessions were offered prior to the interventions (1–5 sessions). One study used the researcher and a doctoral student to deliver the programme.22 The length of the interventions varied from 2 to 10 months and frequency ranged from two to five sessions per week. The session duration varied from 15 to 40 min, with two studies not reporting a specified duration.19 ,24 Six interventions consisted of a structured programme and included: implementing only one GMS per session;17 focusing on a different GMS each week;18 providing a circuit in which children chose their own task and difficulty;23 or a structured programme in combination with either supervised free play or unstructured activities.20 Two studies involved parents in the intervention.18 ,19
Efficacy
The Test of Gross Motor Development 2 (TGMD-2) was the most common measure.17 ,21–24 Six studies reported a statistically significant effect of the intervention.17 ,18 ,20–23 Three studies reported a significant effect on the total scores of motor skills18 ,20 ,21 and three studies reported significant effects on either locomotor skills, object control skills or on individual skills.17 ,20 ,22 ,23
Discussion
This review examined literature published between June 2007 and January 2015 on interventions to improve GMS in young children (0–5 years). Seven studies were included and 86% found evidence that interventions are successful. Since developing GMS has been recommended as part of national physical activity guidelines for this age group in three countries (which have all been released since the original review),24–26 it is interesting that only seven interventions have been reported in the past 8 years. Reasons for a limited implementation of programmes to develop GMS could be: a lack of funding or interest in this area, the complexity of implementing programmes in childcare settings, or a lack of competence and confidence in setting staff.
Implementation
All studies were implemented in early childhood settings. This setting is popular for group RCTs because it is relatively easy to randomise at a whole centre level, and programmes can be incorporated into regular routines. Furthermore, it maximises the number of staff involved and the responsibility of implementation can be shared. Compared to the previous review, the number of RCTs has increased from 29% to 86%, which is positive given that RCTs are the ‘gold standard’ in research design.
Setting staff delivered the intervention in six studies and training was offered to increase their competence and confidence in delivering the programme and to enhance professional development.17–19 ,20 ,21 ,23 This training varied from a 1 day workshop17 ,23 to several separate workshops spread over different days.19 ,20 Professional development of staff is important to enhance their self-efficacy in delivering a programme and to provide them with up-to-date information on the importance of GMS and how to teach them. Especially in young children it is important to enhance their motivation and involvement through people that have experience, are competent and confident. Other advantages of setting staff delivering the intervention have been mentioned in the previous systematic review12 and include maximising the potential sustainability of the programme and minimising costs associated with implementation.
As recommended by Riethmuller et al12 parents should play an important role in developing GMS through role modelling and providing opportunities, encouragement and support.12 ,24 However, only two studies involved parents. This was done through home connection materials such as educational handouts and a music CD18 or parent information sessions to inform them on the benefits of physical activity and how to integrate this within their family environment.19 It is recommended to actively involve parents in centre-based GMS development programmes and encourage them to practice skills in the home environment12 to reinforce the learning that has occurred at the centre and strengthen the relationship between the centre and home setting. Informing and guiding parents in how to practice GMS, the duration of practice and how to motivate their children can be done in several ways such as through information sessions, by handing out home materials or via email and the use of social media.
While only seven studies were identified, the sample sizes, duration and programme content varied widely. Most studies included in this review recruited whole childcare centres, which helps to maximise sample size.
The duration of the programmes varied between 2 and 10 months. Four programmes lasted ≥20 weeks,18 ,20 ,22 ,23 an increase compared with the average of 12 weeks in the previous review. Intervention sessions were delivered between two and five times a week and the average duration of the intervention sessions was around 20 min. On average this gives a greater intervention ‘dose’ compared to the studies in the previous review where there was approximately 1 h of instruction per week. Based on this current evidence it seems that a higher intervention ‘dose’ with at least two sessions a week may contribute to the effectiveness of interventions.
Efficacy
Six studies found significant intervention effects.17 ,18 ,20–23 Even though Bonvin et al19 had high methodological quality, they did not collect any data on the exact amount of daily physical activity time or the use of any specific curriculum, which means the intensity might have been inadequate and there was no control on what activities were done.
Not all studies clearly described their intervention programme which makes it difficult to compare intervention components. Therefore, no key components could be identified that would contribute to a successful intervention.
Methodological quality
Four included articles had high methodological quality. Compared to the review of Riethmuller et al,12 the percentage has increased from <20% to 57%, and the high number of RCTs might have contributed to this. Power calculations have been recommended to ensure that appropriate statistical analyses could be performed.14 However, only two studies conducted a power calculation.19 ,23 A reason why two other included studies did not perform power calculations could be because they were pilot studies and therefore not adequately powered to detect statistical significances.17 ,20 For future studies, however, it is important to conduct power calculations in order to appropriately test the effectiveness of these GMS development programmes in young children.
Strengths and limitations
This review has a number of strengths. These include searching multiple databases, extraction of extensive study details from the articles, methodological quality assessments with high agreement levels and alignment with the PRISMA statement.14 Limitations include the following: the effectiveness of interventions could not be compared because of different instruments that were used to assess GMS, only a small number of updated studies were found, and studies had to be published in English.
Recommendations
Development of GMS in young children is important. When given the opportunity and encouragement to learn and practice GMS, children are able to master these skills before the end of childhood.27 The recommendations made in the previous review are still important:12 utilising a partnership approach in which researchers and childcare staff work together to share responsibilities, minimise the burden and support each other; programme facilitators should be chosen carefully because their competence, confidence and enthusiasm influences children's participation; parents should be involved; conducting sample size calculations to ensure appropriate statistical analysis; and improving the methodological quality of interventions (alignment with the CONSORT or TREND statement).Additionally, the following recommendations can be made:
More high-quality GMS interventions are needed based on the current evidence of relationships between GMS development and other developmental areas and extra funding should be provided to support the development of these interventions.
Intervention components should be clearly described in order to compare the different intervention programmes and determine which components contributed to the effectiveness of the intervention. For future research, this is important in order to implement the most optimal intervention programme.
Based on the current evidence it seems that a higher intervention ‘dose’ with at least two sessions a week may contribute to the effectiveness of interventions.
Consistency in GMS assessment is important to compare results between interventions and conduct meta-analysis.
Conclusion
This review highlights the limited studies evaluated to improve GMS in young children over the past 8 years. This is surprising since the importance of GMS development in young children has been proven and given the recommendations made in the previous review.
Programmes designed to increase the development of GMS have been promising although further research regarding efficacy and the optimal dose of implementation is required. As stated in the previous review, parents play an important role in developing GMS in their children. Up to now, few studies have focused on involving parents and children to increase the development of GMS and therefore, this should be a focus for further research. Also, professional development of the educators in this area should be an important component in future interventions to increase the quality of their practice in early childhood settings.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.