Article Text

Abstract
Background Children and youth are at increased risk of sustaining sport-related concussions. There is a need to develop age-specific tools to evaluate the effects of concussion. The objective of this study was to determine normative values for the Child Sport Concussion Assessment Tool (Child SCAT3) in child athletes and evaluate the symptom scoring agreement between the child and parent.
Methods Child SCAT3 was administered to ice hockey players enrolled in a regional minor hockey association. Statistical analyses were performed to evaluate the differences between child and parent reporting as well as those based on age.
Results 227 athletes (7–12 years of age) completed the Child SCAT3. 29 players reported a history of concussion. For the objective components, the average total Standard Assessment of Concussion adapted to a child version (SAC-C) score of 24.4 was made up by orientation (3.7), immediate memory (12.9), concentration (3.8) and delayed recall (3.9) sections. Average errors in the modified Balance Error Scoring System (BESS) were 1.6, tandem gait time 14.9 s and coordination score 0.95. For the subjective component, children reported an average of eight symptoms and a severity of 11; parents reported seven symptoms with a severity of 9. Overall, children reported higher symptom severity in comparison with their parents. In addition, parents significantly underestimated both physical and sleep-related symptoms in comparison with the children's scores.
Conclusions Results provide representative scores for the Child SCAT3 in young male ice hockey players. Clinicians should be aware that parents tend to underestimate their child's symptoms and symptom severity, particularly in the domains of physical symptoms and sleep. Encouraging objective symptom documentation with sleep or pain diaries, for example, may be useful for reliable clinical assessment in this age group.
- Concussion
- Children
- Hockey
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
Normative total symptom number and symptom severity values for children were higher than reported in the Sport Concussion Assessment Tool (SCAT)2 or SCAT3.
Parents significantly underestimate their child's symptoms and severity.
The objective scores in the Child SCAT3 are similar to the normative scores previously reported for the SCAT3 and SCAT2.
Introduction
Approximately 300 000 sports-related concussions occur each year in the USA.1 This is most likely a conservative estimate as many concussions go undetected due to a lack of recognition or under-reporting of symptoms. In children aged 9–16 years, concussion has been found to be the most common specific injury type in minor hockey, accounting for 18% of all injuries in this age group.2 Concussion rates, particularly in leagues where body checking is allowed, are high (range 4–25 concussions/100 players) with reportedly greater rates in older players (ages 16–21). In studies examining emergency department injury data, 30–50% of all concussions were sport-related.3 ,4 Of these, organised team sports, including ice hockey, account for 25–47% of all youth sport-related concussions.3 Youth, particularly those playing contact sports, with a history of concussion are also at significantly greater risk of future concussions.5 ,6 There is a critical need, therefore, to develop age-specific tools that can be used to quickly guide coaches and health practitioners in their concussion assessment in order to begin providing appropriate care.7
The Sport Concussion Assessment Tool (SCAT) was created after the 2004 International Conference on Concussion in Sport,8 and intended as a standardised tool for rapid (sideline) assessment of suspected concussion.9 The SCAT is one of the most commonly used concussion assessment tools used on the sidelines and in clinics.10 ,11 In 2008, an updated version, the SCAT2, was released which combined aspects from previously validated instruments such as the Glasgow Coma Scale (GCS), a modified Balance Error Scoring System (BESS) and Sideline Assessment of Concussion (SAC).12 ,13 The SCAT2 also included an assessment of symptoms, neurocognitive ability and coordination.9 ,13 More recently, in 2012, after the fourth International Conference on Concussion in Sport, the SCAT3 was released. This updated version was reorganised and the ‘Total Score’ removed, as there was no evidence to support its continued inclusion.13 The SCAT3 includes a background information section followed by symptom evaluation, neurocognitive testing and modified balance/coordination testing.9 While the symptom evaluation remains unchanged from the SCAT2, more emphasis is now placed on differentiating the number of symptoms and their severity to help identify the areas most affected by concussion.13 Concurrent to the SCAT3 release, a children-specific version, the Child SCAT3, was issued as previous studies found that young children (9–10 years) were scoring significantly lower than older children on the cognitive and balance components.14
The Child SCAT3 is specifically designed for children aged 5–12 years. The tool is similar to the SCAT3 but includes a simplified, age-appropriate symptom checklist and a cognitive and balance component.9 Parental symptom reporting is also included as several studies have suggested that information from both child and parent reports should be obtained to provide a more accurate representation of the symptoms.15–17 The purpose of this study is to report normative baseline scores in young children using the Child SCAT3 and to compare child and parent symptom scores. These scores may be useful in assisting health practitioners to focus their clinical assessment on areas of concern.
Methods
Participants
At the beginning of the 2014–2015 season, all players between the ages of 7–12 years of age from a regional minor hockey association in British Columbia were evaluated using the Child SCAT3. Owing to the limited number of female players, only data from the male players were used for the analysis.
Design and data collection
All baseline evaluations took place at a registered athletic therapy clinic in British Columbia. Parents provided written consent, and players provided assent prior to the evaluation. Age-appropriate SCAT3 testing was a mandatory part of the minor hockey association's concussion protocol for all registered players. Evaluations were completed in private rooms by certified athletic therapists, physiotherapists or trained graduate students. Administrators received standardised training in testing procedure prior to data collection. The study was approved by the University of British Columbia's Clinical Research Ethics Board.
Child SCAT3
The Child SCAT3 consists of three components. First, basic background information such as demographics (ie, age, gender, dominant hand, etc), history of concussion, history of headaches or migraines, and learning disability are queried. Second, subjective symptom reporting is completed by both players and their parents. Parental reporting of symptoms is unique to the Child SCAT3. Questions pertaining to the child's cognitive and physical symptomatic experiences are simplified in this version for younger children. Symptom scales are based on a four-point Likert scale.
The third section of the test involves objective testing of cognitive and physical components. The Standard Assessment of Concussion (SAC), adapted to a child version (SAC-C), comprises orientation and concentration subsections. The physical component includes the modified BESS with two trials of stance with eyes closed for 20 s. Each child is first asked to stand with their feet shoulder width apart with their hands on their hips. The second trial involves a tandem stance with the dominant foot in front. Error points are given if the child deviates from the predetermined stance. A maximum of 10 errors is allowed. This is followed by a tandem gait test where the child is asked to walk a 3 m line as accurately and quickly as possible while maintaining a heel-to-toe gait. The final physical component comprises a finger-to-nose coordination test.
Analysis
Descriptive statistics were used to evaluate the data. The mean, SD and range of each of the three components of the SCAT3 were evaluated separately. Subsequently, statistical testing was performed to evaluate the differences between child–parent reporting. Since the data were not normally distributed, non-parametric tests were used. A Wilcoxon signed-rank test was used to evaluate the differences between child and parent reporting for the symptom scores. A Kruskal-Wallis test was used to elucidate significant differences among the major components including: total symptoms, symptom severity, parent symptoms, parent symptom severity, BESS, orientation, immediate memory, concentration, delayed recall and total SAC-C score based on age. A Bonferonni correction was employed to correct for multiple comparisons. Statistical analyses were run using Statistical Package for Social Sciences (SPSS) (V.22.0; SPSS Inc, Chicago, Illinois, USA).
Results
This study included 227 male athletes between the ages of 7 and 12 years (mean 10.4 years). Within this group, 29 athletes had a history of concussion, 6 had a history of migraines and 10 reported a learning disability. The mean Child SCAT3 score for each of the three components is presented in table 1. Overall, the players reported an average of 7.9 symptoms and a severity of 11.4, whereas parents reported 7.2 symptoms with an average total severity of 9.8. The objective component of the Child SCAT3 was divided into cognitive and physical sections. The cognitive section was summarised using the total SAC-C score, with the average being 24.4 out of 30. Average scores on the physical section were 1.6 on the BESS total errors, 14.9 s on tandem gait and 0.95 on the coordination component.
Child SCAT3 average scores and range
The scores for the Child SCAT3 were then stratified by age, with the exception of the children aged 7 and 8 years who were removed from further analysis due to the very low n in this group (n=1, n=4). Data from players between the ages of 9 and 12 years were divided into four subgroups based on age (table 2). No significant differences were found in the scores across the age groups with the exception of the total SAC-C scores between children aged 9 and 12 year with the 9-year-olds scoring significantly lower (p<0.003).
Child SCAT3 and major subsection scores by age (9–12 years)
Analyses were performed to explore differences in child–parent reporting. There were no significant differences between the child and parent reports on the total number of symptoms, but there was a difference between child and parent reporting of symptom severity with parents reporting significantly lower symptom severity (p<0.001; figure 1).

Total symptom number score and symptom severity score for both child and parent. *Significant difference between child and parent (p<0.001).
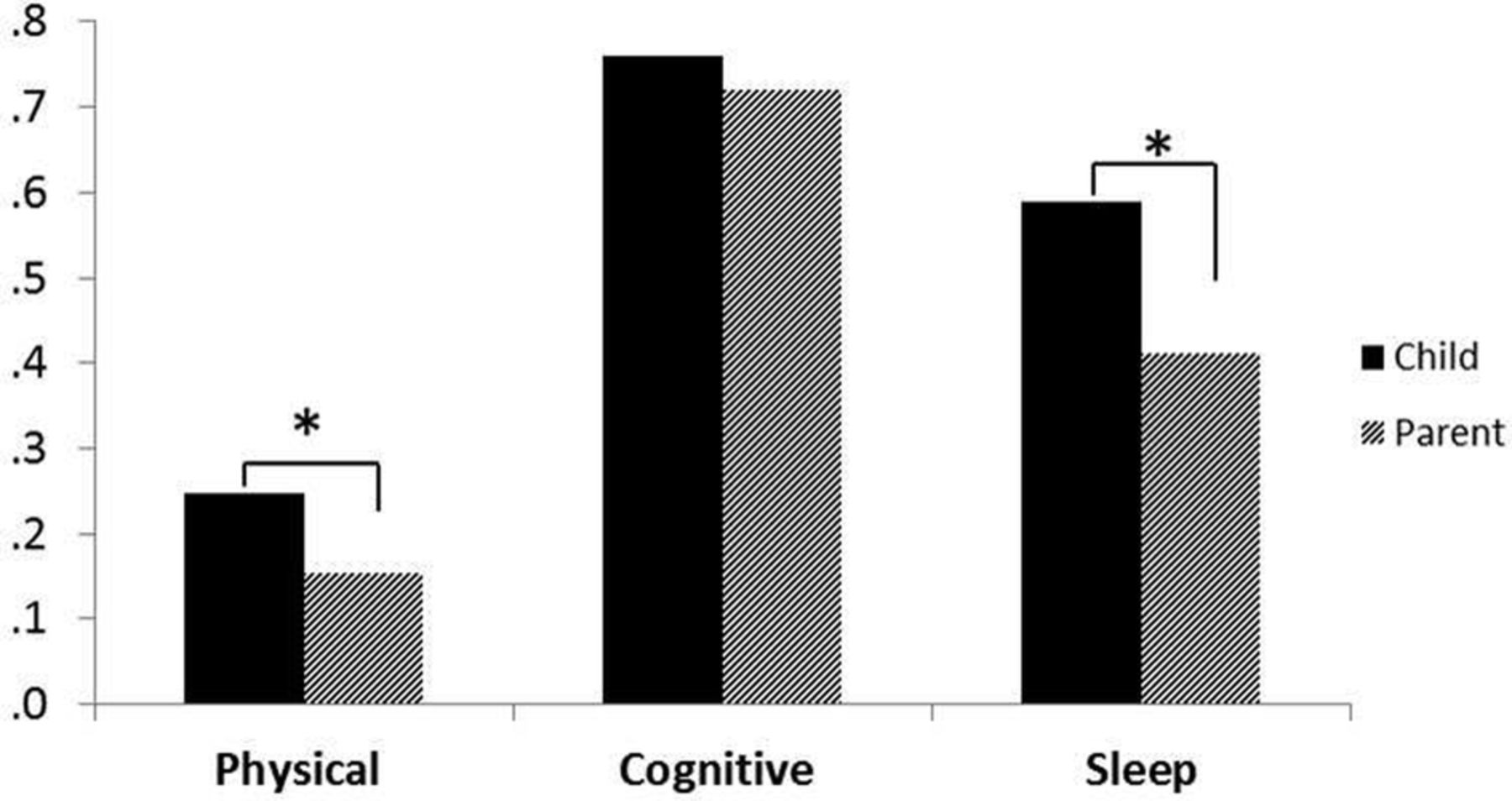
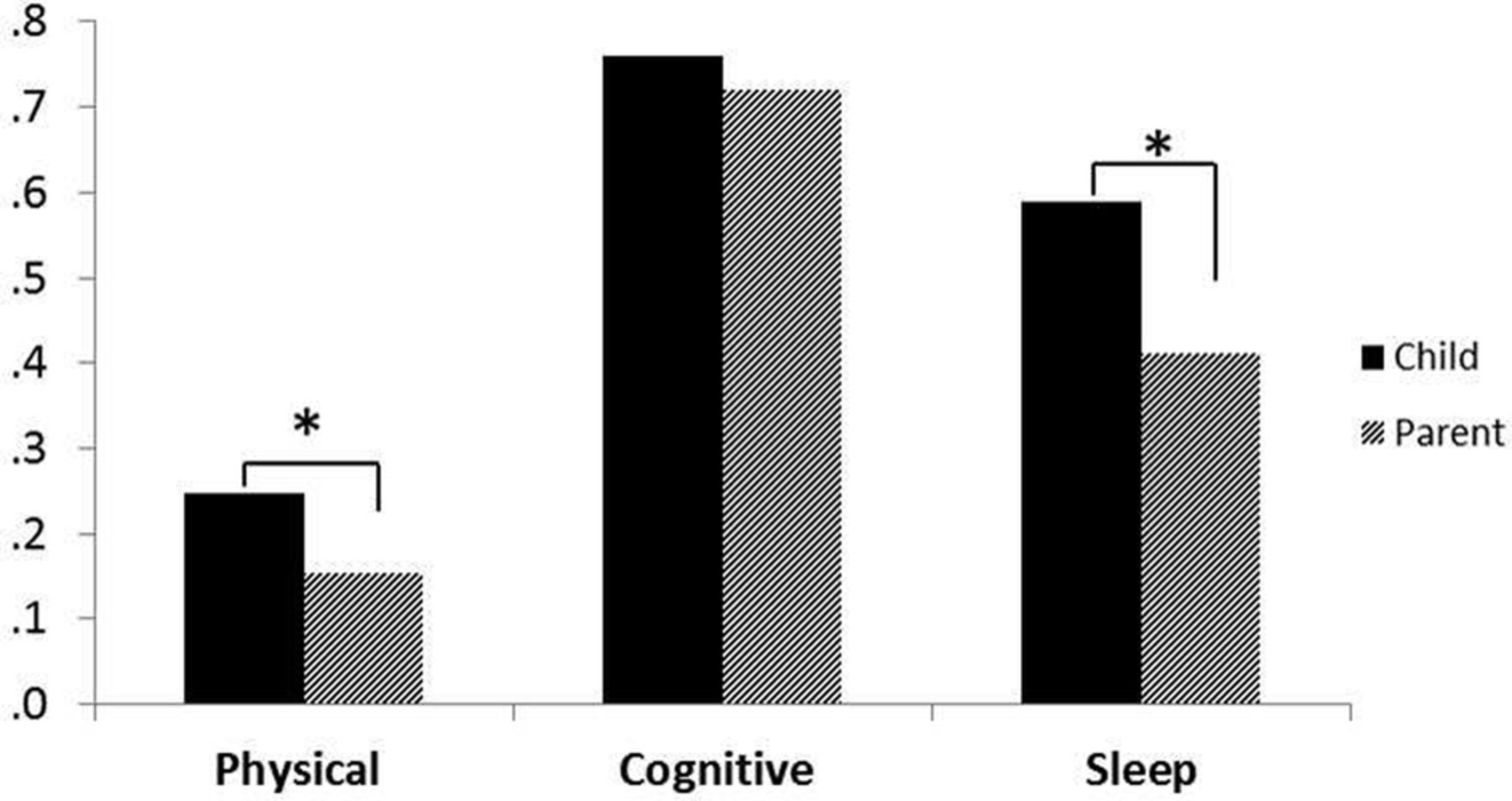
Further analysis of the subjective components was conducted by grouping the symptoms into three clusters: physical, cognitive and sleep.9 The per cent of children and parents reporting symptoms in each cluster is shown in figure 2. Overall, the parents significantly underestimated symptoms in comparison with the children in the physical (p<0.001) and sleep (p<0.001) clusters.
{kind=link}
{kind=link}
Percentage of symptoms reported in each symptom cluster for both children and parents. *Significant difference between child and parent (p<0.001).
Discussion
Since the Child SCAT3 was released following the 2012 International Conference on Sport Concussion, it has been recommended and widely used to evaluate children after a suspected concussion. Tests such as the Child SCAT3 rely on healthy baseline comparisons collected during the preseason to identify and manage concussions.18 However, collecting baseline data is time-consuming and can be a financial strain on volunteer youth organisations. Therefore, establishing baseline values can be an extremely useful reference for health practitioners. Previous studies have been conducted in youth hockey players using the SCAT2; however, the SCAT2 was not recommended for children under the age of 10 years. To our knowledge, this study provides the first normative baseline data for the Child SCAT3 in male child athletes between the ages of 9 and 12 years.
Both the child and parent total symptom number and symptom severity scores in this population are higher than those reported in previous studies using the SCAT2.14 ,19 This increase could be attributed to changes in the symptom reporting question language and scale. The SCAT2 used a seven-point Likert scale ranging from ‘none’, ‘mild’, ‘moderate’ to ‘severe’, while the Child SCAT3 uses a simplified four-point Likert scale ranging from ‘never’, ‘rarely’, ‘sometimes’ to ‘often’. The inclusion of parent reporting provides an additional source of information regarding the child's symptoms. However, the parent reporting must be considered in conjunction with the child reporting as previous research with proxy reporting has shown that parents often under-report the number and severity of symptoms in comparison with their children.20–22
The objective components of the Child SCAT3 consist of the SAC-C, BESS and coordination test. Previous studies had shown a significant age effect for the objective measures with younger athletes scoring significantly lower than older ones. When compared with scores from the SCAT3, collected within the same hockey organisation (Smith-Forrester J, Sun J, Kush C, et al. Sports Concussion Assessment Tool 3 (SCAT3): baseline values in adolescent male ice hockey players. Clin J Sport Med 2015; submitted), there is no longer a significant difference. The SAC-C scores, modified BESS and coordination test are also comparable to those from the older SCAT2.14 These findings support the changes made to the Child SCAT3 to reduce the impact of age on the tool.
Although previous studies have found differences in SCAT2 scores related to age, gender and concussion history, this study focused on the differences pertaining to age as the study population consisted only of young males and only a few of the participants had a history of concussion. Age being the variable of interest, scores were stratified by age to account for the rapid developmental changes that occur in the brain during childhood and adolescence.23 The results showed no significant differences between the age groups for child or parent total symptom number scores, severity scores, BESS or individual SAC-C components. The total SAC-C scores were similar to those from previous studies, however a significant difference remained between the youngest (9-year-olds) and the oldest (12-year-olds) age groups.
We grouped symptoms into three of the four clusters identified in the Zurich consensus statement—physical, cognitive and sleep.9 Significant differences were reported between child and parent reporting for the physical and sleep clusters, with the parent group under-reporting the number of symptoms compared with the child group. No such differences were seen for the cognitive symptoms. This discrepancy in the child–parent agreement could be associated with the developmental stage of the child with various studies showing increasing agreement with age.21 ,24 ,25 It is suggested that clinical observation of behaviour might be more important in younger children who do not have the ability to clearly convey how they are feeling. Importantly, many of these symptoms are not specific to concussion and represent the range of typical behaviour within this age group. Practitioners should be aware of this range so as not to place too much emphasis on these behaviours when assessing concussion.
The SCAT3 and Child SCAT3 were developed for identifying possible concussions and helping to establish return to play protocols. Emery et al found that the rates of concussion in Peewee division hockey (ages 12 and under), where body checking was permitted, were three times higher compared with those where it was not allowed.26 This study, as well as the high rates of concussions in youth hockey, has led Hockey Canada to remove body checking from all minor hockey associations up to and including the Peewee division.27 This policy change is positively reflected in our sample, as only 29 of the 227 athletes (12.8%) reported a previous concussion. This is substantially lower than the 36.4% of Bantam and Midget division players (13–17 years) who reported a history of concussion.28 These findings are similar to the results obtained by Kontos et al29, where younger football players were less likely to suffer a concussion compared with their older counterparts. The demographic information provided in the Child SCAT3 reveals that the majority of the reported concussions in this sample were not a result of playing hockey and there was no significant age effect on the number of previous concussions in this sample.
Limitations
This study had several limitations. First, our sample consisted only of male hockey players. We chose to limit our sample to that group in order to create a more homogeneous population and control for known gender differences. Second, the sample size (n=227) is limited for a normative value study. Nonetheless, we were able to demonstrate statistically meaningful values for our sample population and identify discrepancies between child and parent reporting. Lastly, despite efforts to control for interexaminer interpretation (training, etc), inconsistencies may have been introduced within the data collection process, especially on the objective measures.
Conclusion
This paper provides the first normative baseline values for the Child SCAT3 in young male hockey players. Overall, these findings suggest that the new Child SCAT3 is an appropriate replacement for the SCAT2 in assessing children as young as 9; however, the sensitivity of this tool for identifying possible concussion still needs to be tested. By including parent-reported symptoms, the Child SCAT3 allows for a more complete picture of the child's health. Clinicians should be aware that there are discrepancies between child–parent symptom reporting, particularly in physical and sleep domains. On this basis, clinicians should include both child and parental input as well as ask probing, age-appropriate questions to elicit greater details regarding the child's overall function. Future research is clearly needed to determine the value of this tool in sideline assessments and to clarify the selective advantages of separate parent and child reporting when assessing children who have a suspected concussion.
References
Footnotes
Contributors CK, JS, BB, WJP and NV-B were all involved in the planning of this research study and manuscript. SP, JS-F, NA, JS and NV-B were all involved with conducting the study. SP, JS-F, NA, CK, JS, BB, WJP and NV-B were all involved in the reporting of the data and the writing of this manuscript. NV-B, as the guarantor, is responsible for the overall content of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.