Article Text

Abstract
Background Static stretching (SS) is a recovery intervention used for the reduction of muscle soreness postexercise. The effects of SS on elite young footballers have received little attention, and therefore the aim of this study was to assess the effects of SS on muscle recovery following competitive soccer matches in elite young footballers.
Methods Ten male participants (16±1 years) were recruited from an English Premier League professional soccer academy. Using a controlled crossover design, participants followed one of two recovery interventions (SS or passive recovery (PR)) immediately following completion of competitive soccer matches. Muscle oedema, creatine kinase (CK), countermovement jump with arms (CMJA) performance and perceived muscle soreness were assessed before, immediately after and 48 hours postmatch.
Results Competitive soccer matches significantly induced muscle damage, with time intervals of perceived soreness and CK showing significant increases (p<0.05), and CMJA showing significant decreases between prematch, postmatch and 48 hours postmatch for both SS and PR (p<0.05). Comparisons of the absolute effects of SS with PR only revealed significant decreases for CK 48 hours postmatch (p<0.05) as a result of SS intervention.
Conclusion The current study demonstrated competitive soccer matches induced muscle damage, which may have detrimental effects on future performance within 24–48 hours postmatch. Furthermore, there was limited evidence to suggest SS would assist in the reduction of muscle soreness postexercise. Therefore, it can be argued that SS is not a beneficial recovery option for elite youth soccer players.
- Injury prevention
- Warm-up
- Sport Performance
- Stretching
- Coaching
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Static stretching (SS) is an intervention historically recommended as a recovery method following exercise to prevent or reduce muscle soreness,1 2 often referred to as delayed-onset muscle soreness. When performing SS, muscles are elongated, often to the point of slight discomfort where they are held for a prescribed period of time.3 It has been suggested that SS may assist in the dispersion of postexercise muscle oedema,4 reducing the potential damaging effects of reactive oxygen species, neutrophils, lymphocytes and proinflammatory cytokines which, although act as a protective mechanism, may inadvertently cause further cell damage.5
In addition to the recommendations for using SS with non-elite participants,1 SS is known to be used by elite athletes, with research highlighting the application on national-level basketball4 and soccer3 players. Furthermore, Dadebo et al 6 reported English Premier League football clubs dedicate almost 40% of training time to flexibility training, with the most common technique being SS, although this study did not specify the context in which SS was implemented (warm-up or cool-down).
Applied studies investigating the effects of SS have explored numerous sports such as basketball,4 7 8 Australian rules football9 and soccer.3 10 11 Research assessing the effects of SS in basketball has revealed varied and inconclusive findings. Montgomery et al 7 compared the effects of SS on physical performance markers of basketball players with pretournament baseline values, with SS having no significant effect on performance. These findings are supported by a review study by Calleja-González et al,8 advising against the use of SS as a recovery intervention for improving flexibility and reducing adhesions postcompetition. Limitations to the study produced by Montgomery et al 7 can be highlighted, as data were collected following competitive basketball matches on three consecutive days, suggesting an element of cumulative muscle damage may exist, questioning the transferability of these findings to elite youth soccer as this may not truly represent an expected competitive schedule.
In contrast to research demonstrating SS has no effect on recovery, Delextrat et al 4 report a significant reduction in perceived muscle soreness (PMS) (females) and a significant improvement in countermovement jump with arms (CMJA) performance (males) as a result of an SS intervention on state-level basketball players. Again limitations to this study exist as the recovery intervention incorporated massage therapy, and therefore findings cannot be directly compared with studies focusing solely on SS. Additionally, caution must be taken when assessing the transferability of findings from various sports to soccer, as physical demands between sports are likely to differ, resulting in varying degrees of muscle damage sustained.
In order to truly assess the effects of SS on recovery of soccer players postcompetition, it is important to use soccer players as participants in research studies. Dawson et al 10 reported a significant improvement in peak power 15 hours postexercise when assessing semiprofessional male soccer players; however, no differences in subjective assessments or range of movement were found. These findings may appear more applicable to elite youth soccer; however, athlete training status and participant age (24±3 years) may not truly represent the elite young population. It may be suggested that muscle damage elicited from a competitive semiprofessional soccer match may differ substantially from that experienced at elite standard, therefore affecting the impact of SS as a recovery technique.
In contrast to the findings of Dawson et al,10 Kinugasa and Kilding11 reported SS had no significant effect on non-elite youth soccer players following three soccer matches compared with a control. Despite the use of youth participants (14±1 years), athletes were considered non-elite, again questioning the applicability of findings to the elite youth population. Additional limitations to this study may also be highlighted; first the primary assessment method was subjective, and therefore caution must be taken when considering the effectiveness of SS for recovery based on these results; and second, participants completed three competitive soccer matches within 1 week, and an average of all prematch, postmatch and postrecovery assessments for all matches were calculated and used for statistical analysis. The grouping of all data for statistical analysis may impact the ecological validity of this study as results represent cumulative muscle damage rather than the effects of SS on single trials.
The use of SS as a recovery intervention has been extensively studied, and despite inconclusive findings would appear to be used as a recovery intervention following exercise.3 4 6 To date, limited research has been conducted on the effects of SS as a recovery intervention following competitive soccer matches for elite young soccer players, and with a dearth of research in this area it may be hypothesised that current practices in elite youth soccer are supported by inapplicable evidence. The variance in sports studied and participant training status and age throughout literature does not allow for current research to be applied to the elite youth population; therefore, the aim of this study was to compare the effects of SS with a control of passive recovery (PR) following competitive soccer matches using elite young soccer players.
Methods
Participants
Ten elite young soccer players (mean (±SD): age 16 (1) years, stature 173.5 (6.1) cm, mass 63.3 (6.5) kg) were voluntarily recruited from a professional football academy in the English Premier League to participate in this study. Prior to commencing this study, participants were informed of any risks that may occur, and player and parental consent was obtained. Participants were ensured that any results from testing would be kept confidential and that the findings would not affect their role within the team. All procedures were conducted in accordance with the Declaration of Helsinki, and the study was ethically approved by the Faculty of Science, Engineering and Computing Ethics Committee (Kingston University London, UK).
Experimental design
Participants were required to complete a minimum of three 80 min competitive soccer matches for each recovery intervention (SS or PR). In order to assess the extent of muscle damage elicited from matches, markers of muscle damage (creatine kinase (CK)), CMJA, muscle oedema and PMS were measured before (pre), immediately after (post) and 48 hours after (48 hours post) each competitive soccer match.
Experimental protocol
Physical assessments
On arrival to the match facility, participant stature and mass were recorded, immediately followed by the recording of PMS at 2.5 hours prior to exercise commencing. PMS was indicated using a 10-point visual analogue scale from 0.5 to 5.
Immediately following subjective soreness assessment, muscle oedema was taken using a constant-tension tape measure to assess muscle circumference,12 13 using three sites of the lower body; the two sites on the lower leg of the gastrocnemius were identified by one-third (OedemaG1) and two thirds (OedemaG2) of the lower leg length calculated by the distance from medial condyle of the tibia to the calcaneus tarsal. The site on the upper leg of the quadriceps (OedemaQ) was identified by the midpoint of the distance from the patella to the iliac crest. Following these initial assessments, CK levels were assessed using the i-STAT 1 Analyser (Abbott Point of Care, Abbott Park, Illinois, USA) using fingertip whole-blood samples according to the manufacturer’s instructions. Two hours prior to exercise, CMJA was recorded using the Smart Speed Jump Mat (Fusion Sport).
Recovery intervention
Prior to any participation in matches, a physical and technical preparation warm-up was conducted by a sport scientist and a UEFA-qualified coach, respectively. Warm-ups remained consistent throughout the duration of the study, comprising 15 min physical preparation involving muscle activation, movement preparation and dynamic stretching and mobility, and 15 min of positional and technical football work. For consistency, the warm-ups were conducted by the same sport scientist and coach prior to all competitive games.
Immediately following completion of the competitive games, participants were required to complete either the PR protocol which consisted of 10 min passive seating, or the SS protocol consisting of two 15 s stretches to the gastrocnemius, hamstrings, quadriceps, glutes, hip flexors, adductors and abductors. On completion of the recovery protocols, participants were required to repeat the assessment of muscle damage markers in the same order as was taken prematch. Postmatch assessments were undertaken within 30 min of completing the match. The same assessments of muscle damage were recorded at 48 hours postexercise. On every occasion, the assessments were carried out in the same order and by the same sport scientist. The time intervals of assessments (prematch, postmatch and 48 hours postmatch) were consistent with those used throughout literature.14–16
Player exclusions
For the purpose of control, and for the monitoring of physical outcomes of competitive soccer matches, global positioning systems (GPS) were worn by all the participants when competing in the games. The GPS units (STATSports Viper) report movement variables across all axes, as well as heart rate data. Individual thresholds based on these movement parameters are set according to the average of the combined variables for all full competitive matches completed. As a result, match percentages were calculated, with the average of dynamic stress load, metres per minute, speed intensity, high metabolic power distance, high speed running distance, accelerations, decelerations, heart rate minutes above 85% of max and heart rate exertion over all full games amounting to a match percentage of 100%. This match percentage determined the individual intensity of training and matches completed for all players. To ensure the intensity of each competitive football match remained consistent throughout the study, participants whose match percentage for any particular game was ±10% of their average match percentage for all completed matches were excluded from the data collection for that specific competitive match. Furthermore, participants were excluded from data collection for individual games if they failed to complete a minimum of 80% of the 80 min match, while goalkeepers were excluded from the study due to the inability to control consistency in physical loading for matches.
Statistical analysis
Means and SD of all anthropometric data were recorded, and all data were analysed for normal distribution, with analysis of muscle damage markers only commencing following assessment of normality. The assessment markers recorded were compared across the two conditions (SS and PR) and three time intervals (pre-exercise, postexercise, and 48 hours postexercise) using a within-subjects repeated-measures analysis of variance in statistical software SPSS V.23. Paired samples t-tests were used as posthoc analysis. In case of data with violations in normality, Friedman’s non-parametric statistical test was conducted with a Bonferroni posthoc adjustment. Statistical significance was accepted at p<0.05.
Results
Analysis of data within conditions across time intervals (prematch, postmatch, 48 hours postmatch) produced significant differences (p<0.05) between all time intervals for SS and PR interventions when assessing CK, CMJA and perceived soreness as markers of muscle damage (table 1). Additionally, significant differences were found between pre-exercise and 48 hours postexercise for PR of OedemaG1 (p=0.024, effect size (ES): 0.450, 95% CI −0.054 to 1.334) and OedemaQ (p=0.023), while OedemaQ SS showed significant differences at prematch and immediately postmatch (p=0.028).
Comparison of mean (+SD) physiological, psychological and performance markers of muscle damage at prematch, postmatch and 48 hours postcompetitive soccer match in recovery interventions
Further analysis of results for each assessment method of muscle damage showed no significant difference (p>0.05) between recovery interventions of SS and PR for OedemaG1, OedemaQ, perceived soreness and CMJA (table 1). However, analysis of CK indicated a significant difference between SS and PR interventions 48 hours postmatch (p=0.032, ES: 0.427, 95% CI 0.024 to 0.362), whereas analysis of OedemaG2 showed significant differences between SS and PR immediately postmatch (p=0.029, ES: 0.596, 95% CI −1.047 to −0.073) and 48 hours (p=0.006, ES: 0.642, 95% CI −1.109 to −0.251) following completion of competitive soccer matches.
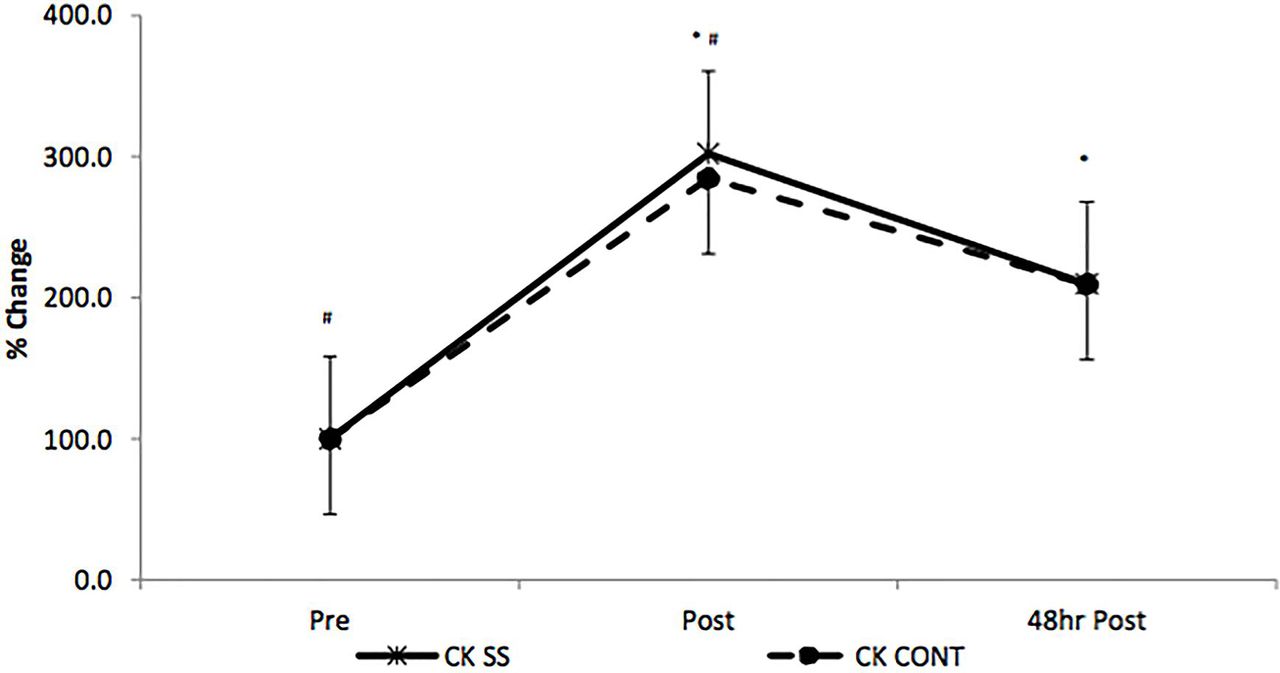
Due to the inter-individual variability of CK, further analysis was conducted to assess the percentage change in CK from precompetition levels at postexercise and 48 hours postexercise between conditions (figure 1). The results show no significant differences (p>0.05) between PR and SS interventions for percentage change; however, a significant difference (p<0.05) across all time intervals was recognised for PR and SS.
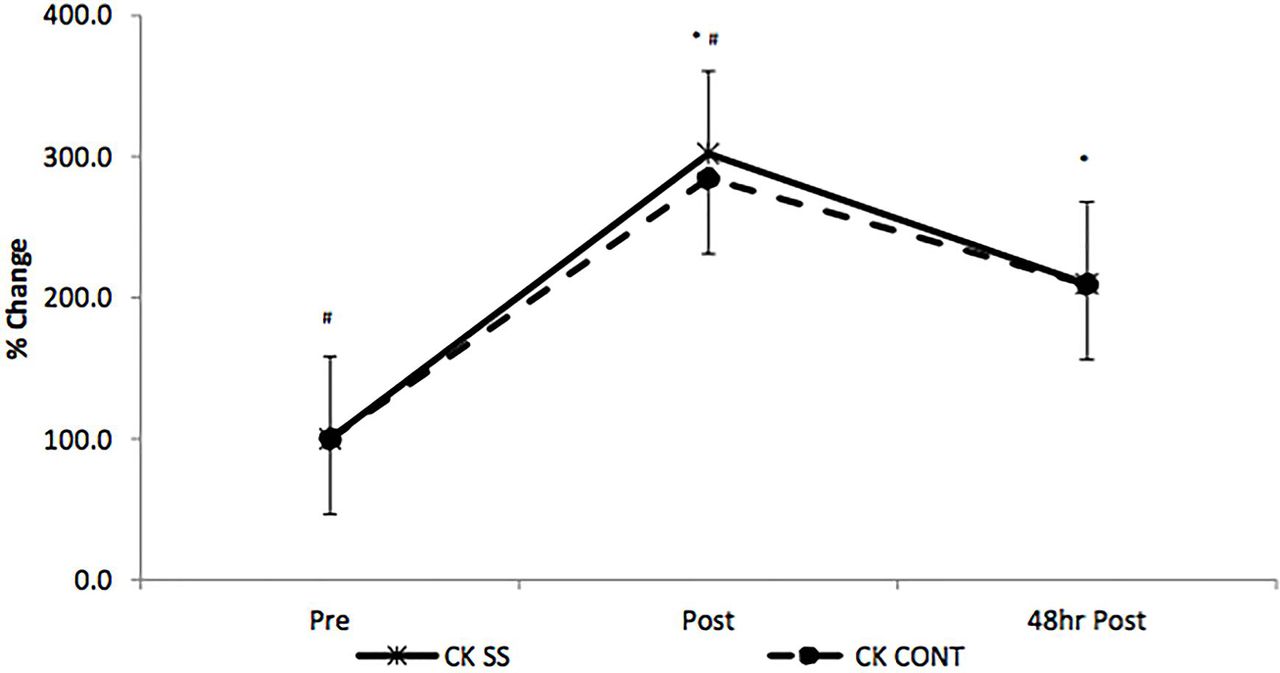
Percentage change in creatine kinase (CK) levels between prematch, immediately postmatch and 48 hours postmatch grouped by condition (SS, static stretching; PR, passive recovery). Error bars represent SE at respective time points. *p<0.05, significantly different from baseline values. #p<0.05, significantly different from 48 hours postexercise values.
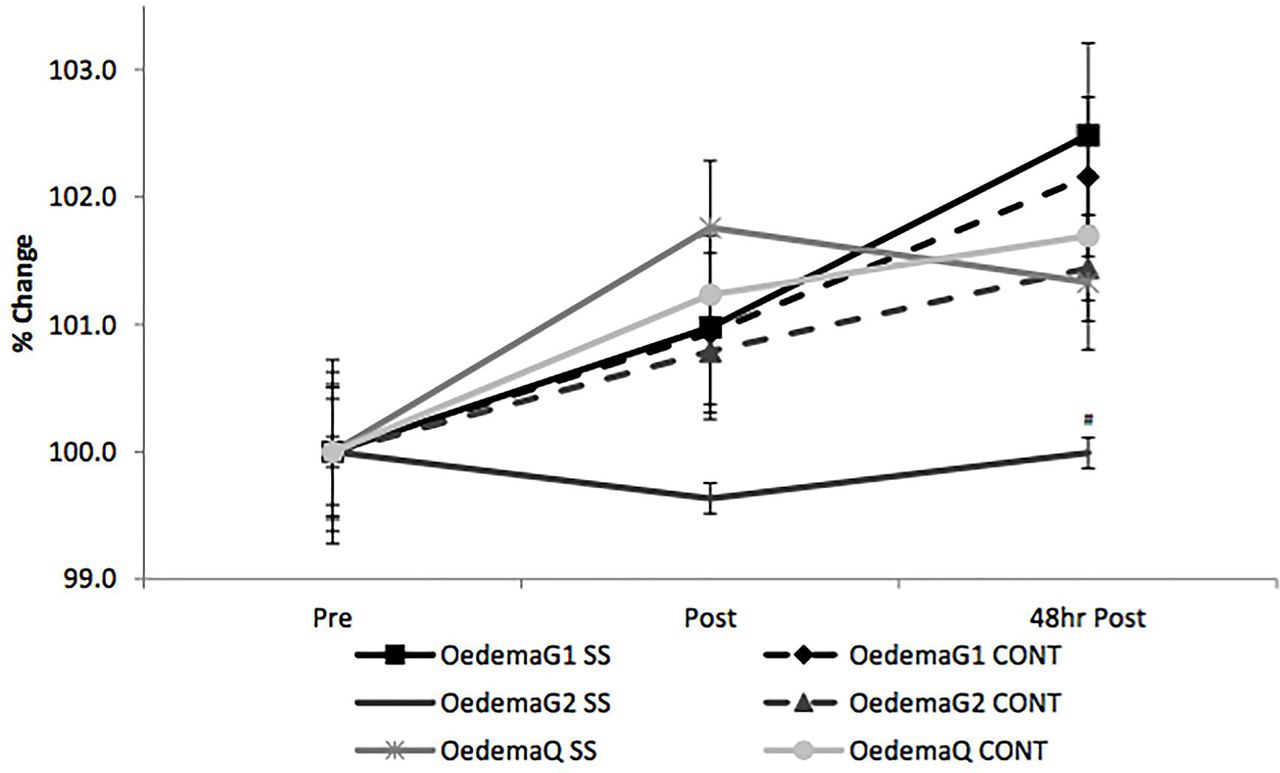
Additionally, the variability between individual measurements of muscle oedema was large, and therefore further analysis was conducted to assess the percentage change in muscle oedema at three lower leg sites from baseline to postexercise and 48 hours postexercise (figure 2). The results show a significant difference (p=0.009, ES: 0.601, 95% CI 0.334 to 1.401) between SS and PR at 48 hours postmatch when measuring OedemaG2. Furthermore, significant differences (p=0.027, ES: 0.440, 95% CI −0.285 to –5.225) were identified across time for OedemaG1 between pre-exercise and 48 hours postexercise when assessing SS, while OedemaQ demonstrated significant differences between prematch and postmatch (SS: p=0.004, ES: 0.716, 95% CI 0.644 to 2.870; PR: p=0.006, ES: 0.714, 95% CI 0.400 to 2.065), and prematch and 48 hours postmatch (SS: p=0.046, ES: 0.726, 95% CI 0.353 to 2.670; PR: p=0.008, ES: 0.647, 95% CI 0.471 to 2.196) for both SS and PR conditions.

{kind=link}
{kind=link}
Percentage change in oedema levels between pre-exercise, immediately postexercise and 48 hours postexercise grouped by condition (SS, static stretching; PR, passive recovery). Error bars represent SE at respective time points. #p<0.05, significantly different from PR.
Discussion
The main findings from the present study showed that competitive soccer matches of elite young soccer players significantly induced muscle damage as demonstrated by the significant increase (p<0.05) in muscle damage markers immediately postmatch when compared with baseline values (table 1). Furthermore, this study demonstrated muscle damage was evident for at least 48 hours postmatch as indicated by the significant difference in muscle damage markers recorded at this time point (p<0.05) in comparison with baseline values (table 1). These findings differ from those of Dawson et al,10 whose results showed a significant increase in PMS only, at 15 hours postmatch and 48 hours postmatch in comparison with baseline values, with no significant differences in performance measures, therefore suggesting soccer matches of semiprofessional soccer players do not elicit significant muscle damage. Additionally, Kinugasa and Kilding11 reported no significant differences in muscle damage markers across time intervals when assessing perceived soreness and performance measures following competitive matches of non-elite youth soccer players. The findings of the current study may therefore suggest that the intensity of competitive soccer matches at elite standard is higher than non-elite and semiprofessional matches, and as a result elicit significant occurrences of muscle damage. These findings present new information on the effects of competitive soccer matches for elite young soccer players.
Further examination of the data from the present study demonstrated a significant reduction in perceived soreness, CK and CMJA assessments between immediately postmatch and 48 hours postmatch, suggesting that although competitive soccer matches elicit muscle damage postmatch, at 48 hours the recovery process had begun and values were returning to baseline for both PR and SS. That being said, the report of a significant difference between pre-exercise and 48 hours postexercise for perceived soreness, CK and CMJA may suggest that the body is going through a process of repair and regeneration,17 and a return to optimal performance levels is yet to be achieved, presenting new information on the recovery process of elite young athletes in the days following competitive soccer matches, and may prove useful to coaches preparing training sessions at 48 hours postmatch.
Comparisons between SS and PR show no significant differences for OedemaG1, OedemaQ, perceived soreness and CMJA (p>0.05). These results are consistent with previous research suggesting SS as a recovery technique has no effect on recovery time when considering muscle oedema,18 perceived soreness10 11 18 and CMJA7 10; therefore, it may be argued that in contrast to findings by Delextrat et al,4 SS is an ineffective method for reducing muscle oedema for elite young soccer players. Additionally, due to the elite training status of these individuals, the body may be accustomed to managing the repair of damaged muscle fibres and the removal of myoprotein,19 and as a result SS has little effect on the repair process.
However, in contrast to Gill et al,20 CK was significantly elevated (p=0.032) 48 hours postmatch as a result of no recovery intervention when compared with SS. Although this may suggest SS significantly reduces CK following exercise (p<0.05), it may be possible that the individual variability of CK levels at baseline may have an influence on statistical interrogation of results postmatch; therefore, the CK values were aligned for relative change to baseline and expressed as a percentage. Statistical analysis in this form showed no significant differences between SS and PR (figure 1), similar to findings of previous studies.3 11
Analysis of OedemaG2 also showed significant differences between SS and PR interventions immediately postmatch and 48 hours postmatch. Again this contrasts the findings in current literature3 10 11; however, when assessing these results, considerations of compulsory attire of soccer players must be taken into account. The assessment of OedemaG2 was taken at the upper third of the gastrocnemius, an area potentially compressed by the wearing of supportive tape. This may provide a compression aid, which could not be avoided due to the applied nature of this study. As participant use of supportive tape was not recorded, it cannot be assumed that it was used across both recovery interventions, and as such the effects of strappings cannot be directly determined. Again in order to reduce inter-individual variability in muscle oedema measures, manipulation of data to percentage change allowed for further statistical analysis. Results from this analysis (figure 2) showed a significant difference between SS and PR of OedemaG2 at 48 hours postmatch (p<0.05). Again the potential influence of the supportive tape may have a contribution to the results, leading to the significant difference.20
In conclusion the results of this study indicate that competitive soccer matches of elite young soccer players significantly induce muscle damage, and muscle damage markers remain elevated at 48 hours postmatch. Furthermore, the use of SS showed no significant reduction in muscle damage markers when compared with PR following competitive soccer matches. This supports the advice provided by Calleja-González et al, 8 who warn against the use of SS as a recovery intervention for reducing muscle damage postcompetition.
Practical implications
In light of these findings, it may be advised that the use of SS following competitive soccer matches for elite young athletes provides no definitive recovery effect, and that alternative postmatch recovery interventions may be advised. In the applied settings of elite academy football, situations such as away fixtures provide little opportunity for alternative recovery interventions to be implemented postmatch, and as such in these situations it may be recommended that training sessions in the days following (at least 48 hours postexercise) have a reduced load.
What are the findings?
Completion of a minimum of 80% of 80 min competitive soccer matches of elite youth soccer players significantly induced muscle damage.
As a result of muscle damage sustained from competitive soccer matches, elite youth soccer players are in the process of recovery for at least 48 hours postmatch.
Static stretching provides little or no recovery benefit for elite young soccer players following competitive soccer matches when compared with passive recovery.
References
Footnotes
Acknowledgements The authors wish to thank all the participants who volunteered their time for this study and in doing so made the completion of this research possible.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Kingston University.
Provenance and peer review Not commissioned; externally peer reviewed.