Article Text

Abstract
Background and aim Despite evidence of their efficacy, there is no widespread adoption of injury prevention exercise programmes (IPEPs) among young players and coaches in community rugby union. The purpose of this study was to (1) analyse the knowledge and perceptions of injury prevention and IPEPs among staff, parents and players in youth rugby union and (2) explore the facilitators and barriers to implementation of IPEPs. With this contextual information, tailored implementation strategies can be created.
Methods Participants completed an online survey addressing knowledge and perceptions of injury risk, injury prevention practices and a rugby-specific IPEP. Community rugby union players aged 14–18 years, their parents and staff were invited to participate, including school-based and development squads competing at a national level.
Results Surveys were completed by 18 staff members, 72 parents and 56 players. Staff, parents and players believe that the risk of injury in youth rugby union is high and that injury prevention is important. The perceived role in injury prevention and availability of allied health staff, particularly strength and conditioning coaches, was apparent in this sample. Reported barriers to completion of IPEPs related to time, resources, awareness of the programme and end-users' attitudes or motivations. Leadership, the use of role models and the structure and routine provided by an IPEP were considered facilitative.
Conclusions These findings inform future implementation strategies for IPEPs in this setting, including the need to provide practical solutions, education and considering the role of allied health staff in facilitating such programmes.
- injury
- rugby
- adolescent
- implementation
- prevention
Data availability statement
Data are available on reasonable request. Data may be supplied in an unidentifiable format on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In youth rugby union, there is a belief that the risk of injury is high and that injuries can be prevented; however, successful implementation of injury prevention exercise programmes (IPEPs) in ball sports is limited by barriers such as lack of time, resources and player or staff attitude and motivation.
WHAT THIS STUDY ADDS
This study highlights the knowledge and perceptions of parents, in addition to previously reported findings from staff and players, of which there is limited research in a youth rugby union setting.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Practical strategies to overcome logistical barriers may enhance the adoption of IPEPs.
Including allied health staff in education and implementation activities and identifying role models may be facilitative.
Introduction
Childhood injury associated with sport is common and has short-term implications for the individual, their family and sporting team, and their future health and participation in exercise.1–3 Surveillance of 3585 Australian rugby union (hereafter referred to as rugby) players in a school-level competition showed an overall injury rate of 23.7/1000 player hours, with a spike of injuries at the age of 14 years.4 In New Zealand community rugby union, for the 13–17 years age group, players had a 35% chance that at least one injury claim would be made with the Accident Compensation Corporation during a playing season.5 The frequency of injury and potential for long-lasting impact make successfully translating injury prevention research into practice for young community players essential. One method of reducing injury in team sports is using injury prevention exercise programmes (IPEPs), which are effective, particularly when employing strength, balance6 and plyometric exercises.1 In a systematic review and meta-analysis including 27 561 participants aged 10–17 years, the effect of exercise-based injury prevention programmes in organised sports resulted in an injury reduction of 46%.1 In rugby, similar programmes cover a range of injury prevention and safety behaviours targeting spinal injuries, injury during contact, concussion, injury management, warming up and protective equipment.7 8
The efficacy of a rugby-specific IPEP in a school setting was established in a large-scale randomised controlled trial including players aged 14–18 years.9 Designed to be performed at the beginning of a training session or match, when completed at least three times per week, the programme resulted in 72% fewer match injuries overall and a 59% reduction in concussion incidence.9 However, the intention-to-treat analysis showed unclear effects on overall match injuries due to poor compliance. This demonstrates how important it is that the programme is performed as intended. Implementation frameworks guide aspects of implementation that need to be considered in a complex community environment,10 11 one of which is the RE-AIM framework.11–13 This framework measures Reach, Efficacy/Effectiveness, Adoption, Implementation and Maintenance. Evidence exists regarding the reach and effectiveness of IPEPs in rugby,8 14 but if injury prevention strategies are not performed as intended in the community, then similar outcomes cannot be achieved.7 13
Stakeholders’ attitudes and beliefs regarding injury risk and prevention are important to understand, as they play a role in the adoption of IPEPs.15 The Health-belief model outlines the dimensions of perceived susceptibility, perceived severity, perceived benefits and perceived barriers as determinants of the adoption of safety behaviours.16 This study aimed to describe staff members’, players’ and parents’ knowledge and perceptions of injury risk, injury severity and injury prevention in youth rugby union in Australia and explore facilitators and barriers to performing an IPEP. With this insight, implementation planning can be tailored to suit the needs of this population to help bridge the gap between effective interventions and implementation.
Methods
Participants
Parents and staff of rugby players aged 14–18 years were invited to answer a survey between 21 October 2019 and 12 March 2020 in Australia. The teams of interest participated in an interschool competition or state-based squads (Under 16 and Under 19) competing in a national competition.
Survey
The survey created on Qualtrics (Provo, Utah) Online Survey Software was distributed through an invitation email to all players, their parents and staff, including coaches, doctors, physiotherapists, strength and conditioning staff and team managers. Informed consent was obtained from all participants and a parent or guardian of participants <18 years of age.
The survey questions included (1) demographics, competition logistics and resources (9 questions); (2) knowledge and perceptions of injuries and injury prevention in rugby (21 questions) and (3) knowledge and perceptions of a rugby-specific IPEP (15 questions). Sections 2 and 3 were informed by previously described surveys and modified for a rugby setting.17 18 The survey was then assessed for face validity, scope and clarity in consultation with experts in rugby, concussion and sports medicine and trialled by rugby management staff that were not eligible participants, as they did not work at the youth level. The IPEP was described as ‘performing a rugby union specific balance, agility and strength warm-up programme, two to three times a week, for 20 min before matches and training sessions’, with details of the space and equipment requirements. The survey included multiple-choice questions, both single answer and up to three selections, and questions scored on an ordinal 5-point Likert scale.19 For example, (1) strongly agree, (2) agree, (3) neither agree nor disagree, (4) disagree, (5) strongly disagree. Participants were invited to describe their perceived facilitators and barriers and provide feedback on previous experience using IPEPs using multiple-choice and free-text questions. Where a participant had completed <20% of the survey, their response was deemed incomplete and not included in analyses.
Data analysis
Multiple-choice questions were analysed using descriptive statistics and displayed as the percentage of respondents in the category (staff, parent or player) that nominated each response. Where questions allow more than one response, these percentages can add >100%. After reading all of the responses and identifying patterns of feedback, free-text responses to the open-ended questions regarding barriers and facilitators underwent thematic analysis.20 Some of these examples are provided within their nominated theme.
Patient and public involvement
Patients and the public were not invited to comment on the study design, assess the burden of participation or contribute to data analysis or the preparation of the manuscript. The survey was disseminated by representatives of the participating schools and staff of Rugby Australia.
Results
Participants
A total of 18 staff, 72 parents and 56 players completed the survey, with a mean age of 37, 44 and 16 years, respectively. The sample included Under 16 and Under 19 state-based squads, one public school and two private schools, with a response rate of 7.3% (146/2010). Characteristics of respondents are detailed in table 1.
Characteristics of respondents (n=146)
Beliefs and attitudes about injury and injury prevention in rugby union
When asked to rate overall injury risk in youth rugby union, most participants selected ‘high’ or ‘extremely high’. Among the staff, many agreed or strongly agreed that, in general, injuries are preventable (44.5%). However, nearly as many neither agreed or disagreed (38.9%). A smaller proportion of parents (30.6%) and players (39.3%) agreed that injuries are preventable, again with an equivalent number neither agreeing nor disagreeing (30.6%, 39.3%). However, reducing a player’s risk of injury was rated as ‘very important’ or ‘absolutely essential’ by 94.4% of staff, 90.3% of parents and 78.6% of players.
Concussion, knee ligament injury and a broken bone were rated as ‘serious’ by most respondents. Notably, concussion was given the highest rating (‘very serious’) on a 5-point Likert scale by 67% of staff and 69% of parents, but only 23% of players.
The percentage of respondents indicating who they consider responsible for administering injury prevention programmes is shown in figure 1.

The percentage reported by parents, staff and players for who they consider responsible for administering injury prevention programmes in a youth rugby union setting. Up to three responses were allowed.
All but one staff member selected the strength and conditioning/fitness coach as the most appropriate person, followed by the physiotherapist and coach. The majority of players indicated the coach, strength and conditioning coach and physiotherapist roles, with parents allocating the sports teacher as also playing a role in injury prevention. In this sample, in all but the 14-year-old school group (48.0%), two-thirds or more (70.6%–100%) indicated that they had access to a strength and conditioning coach during training sessions. Access to a physiotherapist during training sessions was indicated by a majority of respondents in all but the 15-year-old school category (46.4%), becoming increasingly common in the 16-year-old and open school groups (70.6% and 80.0%, respectively). State-based squads largely had access to both staff members in Under 16 (86.4%) and Under 19 (100%).
Barriers and facilitators
Barriers identified by respondents are shown in figure 2.

The percentage of respondents who selected each barrier to use an injury prevention exercise programme (IPEP). Multiple selections were allowed.
The leading barriers across all respondent groups were poor attitude or motivation of players (67.8%), poor attitude or motivation of staff (45.2%), time constraints (43.8%), lack of awareness of programmes (40.4%) and poor punctuality or player attendance (34.9%).
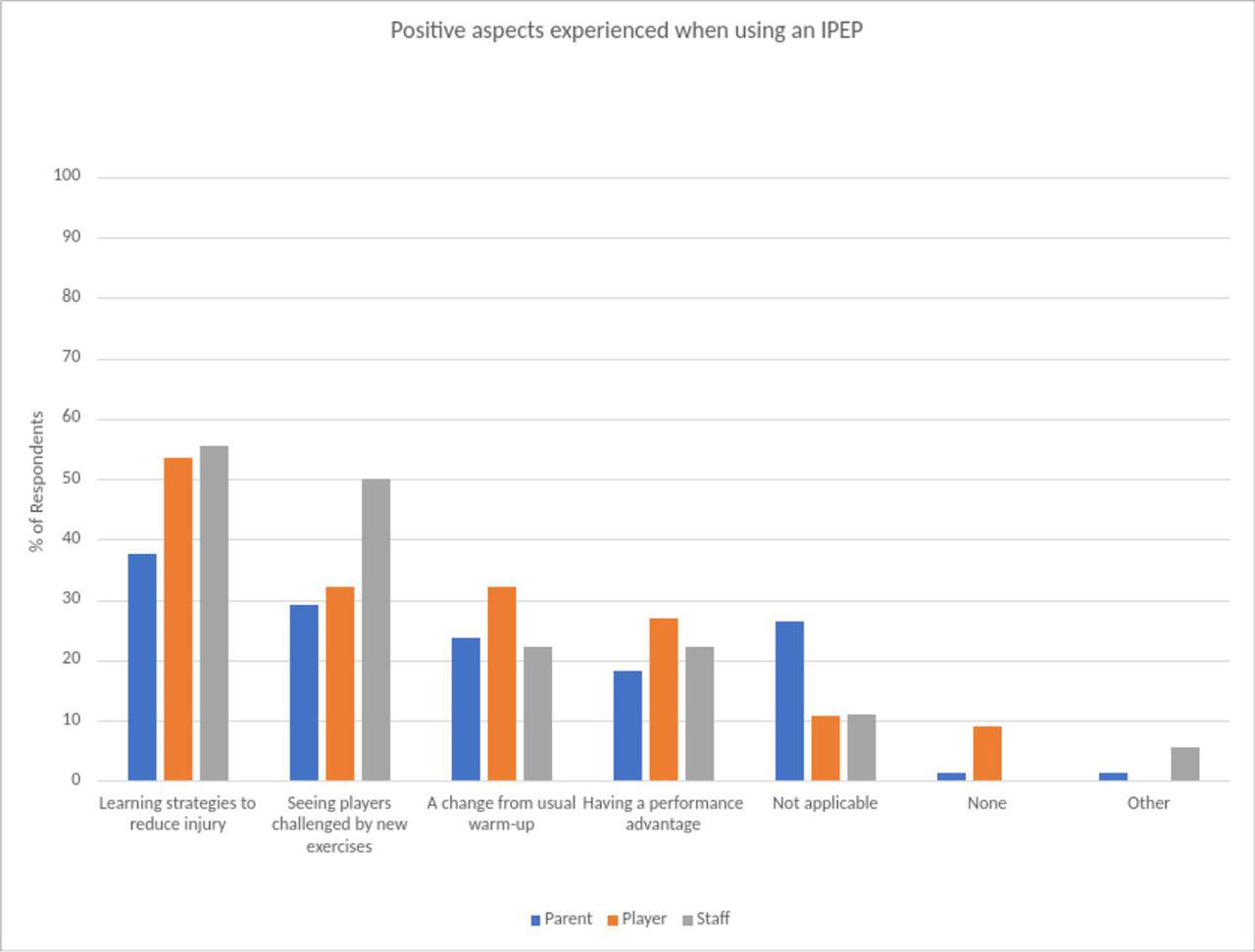
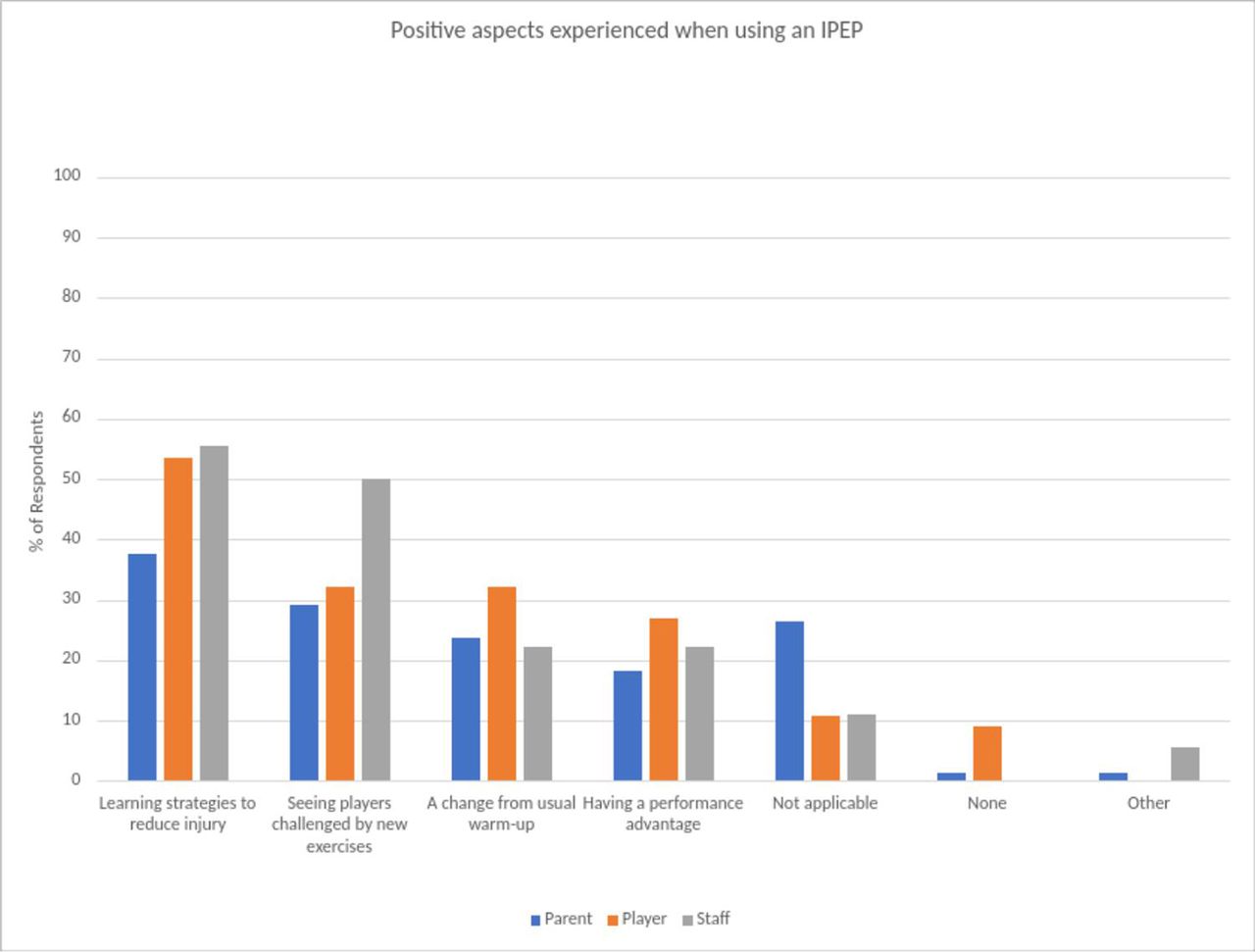
Positive aspects experienced when using IPEPs selected by respondents are shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
The percentage of respondents who selected each positive aspect they experienced regarding available injury prevention exercise programmes (IPEPs). Multiple selections were allowed.
Participants provided free-text responses regarding barriers (86 responses) and facilitators (88 responses) to completing an IPEP. Examples are shown in boxes 1 and 2.
Examples of barriers to using an injury prevention exercise programme reported by respondents in free-text responses, summarised and categorised into themes
Theme
Poor attitude or motivation of the players
Lack of interest
Lack of commitment and concentration
Engagement, taking it ‘as a joke’
Lack of incentive (extrinsic motivation)
Limitations related to the programme
“We just want to have fun”
Lack of interesting activities
Lack of variation
Poor attitude or motivation of staff
Coach not ‘buying in’
Lack of enthusiasm
Lack of incentive (extrinsic motivation)
Culture and tradition (resistance to change from current practice)
Lack of leadership in implementation of the programme
“The coach didn’t watch us”
No direction
Not making a plan
Coordination and organisation
Examples of facilitators to using an injury prevention exercise programme as reported by respondents in free-text responses, summarised and categorised into themes
Theme
Positive behaviour change through the use of structure and routine
A part of the normal routine
Put into the schedule
Incorporating the programme into the training session
Getting ‘into the rhythm of it’
If it happened often, we would get used to it
Consistency
Doing the same thing every day in a structured way
Strong leadership displayed by coaches and/or administration with the creation of rules or policy
Setting standards at the beginning of the season
No warm-up, no play
Run and supervised by the coach
Making it school policy
Making it mandatory
Disciplinary action for failure to complete
Leadership through positive role modelling
Being driven by senior players
Having professional players demonstrate it
Having all players do it/if the whole team is involved
Positive attitude of the players
Discipline
Focus
Positive attitude of the staff
‘Buy in’
Discipline
Coaches realise how valuable it is
There was variation between staff, parent and player free-text responses when they focused on facilitators. Staff reported access to space and equipment (22.2%), punctuality (22.2%) and a positive attitude or motivation of staff (22.2%). Parents and players indicated that the use of structure and routine was a facilitator (17.9%), strong leadership (12.5%), sufficient time (4.7%) and a positive attitude or motivation of the players (4.7%). Of note, players and parents considered having an example set by their peers or professional rugby players to be a facilitator.
Only 2% of respondents, all from a school programme, reported that they had only one field-based training session per week, which, in addition to a weekly match, would not allow the team to complete the IPEP three times a week as a supervised group.
Discussion
There is a lack of evidence on the implementation context and the barriers and facilitators that impact the translation of research into practice.11 21 This is particularly true in community rugby, specifically in the adolescent sphere. To influence the adoption of a programme, first, we need to understand all relevant stakeholders’ knowledge and attitudes that drive injury prevention decisions and behaviour.10 15 Owoeye et al highlights the need for dissemination and implementation research to consider the broad contextual factors that influence injury prevention behaviour, as well as the complex interactions between these.22
This study describes the perceptions of the players as end-users and other actors, such as parents and staff, who are potential influencers on the effectiveness of prevention strategies.22 23 The role of other staff members in addition to the coach was apparent in this population. Identified barriers to adoption and implementation included awareness of the programme and practical factors such as time, punctuality, space and equipment. Another common theme was the attitudes or motivations of end-users. Facilitators included strong and effective leadership, the use of role models, peer support and focusing on structure and routine, which is a strength of IPEPs designed to be used as an alternative warm-up.
Perceived susceptibility to injury and injury seriousness can influence injury prevention behaviours.15 This survey suggests that there is a belief that the risk of injury is high and that injury prevention is of high importance in this context. However, a lack of incentive was indicated as a barrier to IPEP adoption, despite their potential for injury prevention. This is consistent with findings in rugby players in English schools, where injury risk was also perceived as high, with coaches agreeing more frequently than players that injuries can be prevented.24 Both concussion and knee ligament injuries were considered particularly serious by this group. Emphasising injury reductions in these areas addresses an important issue for end-users and may incentivise and influence their decision to adopt an injury prevention programme.25 There was a varied agreement regarding the ability of rugby union injuries to be prevented. However, this may reflect the interpretation of the survey question, which did not define whether this applied to all rugby injuries or select injuries: “In general, do you think that youth rugby union injuries are preventable”.
Awareness of the evidence supporting a programme was considered facilitative by 3.4% of respondents in this study and has been noted in other ball sports.26 A stakeholder’s perception of the quality and strength of evidence that supports a programme’s ability to reduce injury was noted as a key facilitator in focus groups evaluating the iSPRINT school-based physical education programme.27 Norcross et al highlighted a need to demonstrate the relative advantage over current warm-up practices when influencing adoption among high school soccer and basketball coaches.25 This may assist with obtaining ‘buy-in’, a concept that multiple respondents specified.
At a community level, research in other ball sports has focused on coaches as the delivery agents of IPEPs.17 26 28 However, the availability of and perception of the role of allied health staff in administering IPEPs was evident in this cohort. Access to these staff will vary across community settings. Brown et al found that most rugby players chose either the coach or physiotherapist as preferred education sources on injury prevention, including warming up.29 In elite youth football, fitness coaches were observed to be the primary programme deliverers with the support of physiotherapists.30 Dedicating a staff member other than the coach to warm-up may improve player supervision and motivation, and reinforce the structure and routine suggested as facilitators by respondents. Strength and conditioning coaches’ and physiotherapists’ skill sets include teaching correct exercise techniques, which may also improve exercise fidelity. This was low in youth floorball participants, with only three of five exercises completed according to instructions.31 While coaches remain key drivers of IPEPs in rugby,24 where available, the role of allied health staff should be considered, to improve adoption, implementation and maintenance.
Lack of time24 and poor staff and player attitude and motivation are commonly cited barriers in previous research in ball sports.25 26 28 Practical training and directly addressing these concerns in education efforts could assist in overcoming these barriers.32 Lack of time was the third most often cited barrier to completing an IPEP in this study. This may be partly attributed to players’ poor punctuality and a frequently identified barrier, effectively shortening training sessions. Education should reinforce that the IPEP is intended as an alternative to current warm-up strategies, as incorporating an intervention into regular training sessions has been cited as a facilitator and shown to improve compliance.21 28 In particular, punctuality is largely controlled by parents and players once coaches establish clear expectations and standards. Given the expressed importance of injury prevention to parents and players, existing communication channels such as newsletters could be used to deliver key messages when launching an IPEP, which may differ from those targeted at coaches.9
A dose-effect response was demonstrated when using the Activate IPEP. Compared with twice weekly, there were 39% fewer match injuries in those that completed three or more sessions a week.9 In this cohort, the opportunity for sufficient frequency of exposure is not a significant barrier, given that only 2% of respondents had less than three total matches or training sessions per week.
Poor player attitude and motivation rated highly as a barrier, with free-text responses indicating the need for programmes to be fun and engaging. In particular, it was desired that the content of IPEPs includes exercise variation and progression and that they are rugby-specific, similar to previous soccer study findings.26 33 Barden et al identified player and coach concerns regarding a lack of ball work and player enjoyment of the programme.24 The perceived need for the programmes may be improved if education addresses players’ desire to play without restriction from injury and the use of role models.12 34
The theme of leadership was more prevalent among the parents’ and players’ group, with statements referring to both policy creation and the coach’s actions. Supervising and motivating players, setting standards, rules such as ‘no warm-up, no play’, planning and organisation featured in responses. Another leadership opportunity that impacts the motivation of players and staff is role-modelling.12 34 35 Resources could include images and video footage of appropriate role models at an organisational level. Although both professional players and senior players demonstrating the programme were suggested as facilitators in survey responses, electing to use elite sportspeople should be approached with caution. The participant needs to be able to identify closely with the role model to effect behavioural change.35 The Open squad and the Captains are leaders among their peers at the school level. They could be used to demonstrate the programme in training and lead by example, particularly if a highly visible location is available on match day.
This study was limited as it was a cross-sectional survey that is descriptive in nature, with a poor response rate, contributed to by the need for parental consent before distributing to minors. Generalisation needs to be undertaken with caution. There was, however, representation across a variety of school and development squad settings. The results may also be affected by non-response bias with incomplete survey data not included in the analysis. The inclusion of parents as potential influencers and participants in both interschool and national competitions was a strength of this study and the use of both multiple-choice and free-text responses to enrich the qualitative data.
Future research could address the effectiveness of implementation strategies using postseason surveys and data collection regarding attitudes, adoption, compliance and correct execution of the IPEP. Long-term studies are needed to assess factors that influence the maintenance phase and address the different ecological levels within the RE-AIM Sports Setting Matrix,11 including the impact of policy. Focus groups, interviews and concept mapping30 approaches are alternative methods for evaluating participant knowledge and beliefs. The role of a mobile application in both programme guidance and data collection to track compliance and progression may be of interest.
Conclusion
This study has identified features of the current implementation context, injury prevention knowledge, perceptions of responsibility for injury prevention and barriers to implementing IPEPs in youth rugby union. Staff, parents and players agree that the risk of injury is high, that injuries can be serious and that preventing injury is important. Allied health staff such as strength and conditioning coaches should be considered a viable alternative to coaches where available, although coaches remain key influencers and leaders in this setting. Facilitators and barriers are in agreement with other ball sports. However, further research is required to understand how to best influence the behaviour of key drivers and sustain programme use. These findings may be used to inform education and implementation strategies to enable the real-world effectiveness of these programmes.
Data availability statement
Data are available on reasonable request. Data may be supplied in an unidentifiable format on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by University of New South Wales’ Human Research and Ethics Committee (HC190271). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors NS conceptualised the study, reviewed the literature, designed the questionnaire and led the writing of the manuscript. NS is the guarantor for this study. MS completed the questionnaire on Qualtrics, assisted the methods section and conducted analysis. All authors critically revised the manuscript, provided feedback and approved the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.