Article Text

Abstract
Objective Telehealth has been established as a viable option for improved access and timeliness of care. Physician-guided patient self-evaluation may improve the viability of telehealth evaluation; however, there are little data evaluating the efficacy of self-administered examination (SAE). This study aims to compare the diagnostic accuracy of a patient SAE to a traditional standardised clinical examination (SCE) for evaluation of femoroacetabular impingement syndrome (FAIS).
Methods 75 patients seeking care for hip-related pain were included for participation. All patients underwent both SAE and SCE and were randomised to the order of the examinations. Diagnostic accuracy statistics were calculated for both examination group for a final diagnosis of FAIS. Mean diagnostic accuracy results for each group were then compared using Mann-Whitney U non-parametric tests.
Results The diagnostic accuracy of individual SAE and SCE manoeuvres varied widely. Both SAE and SCE demonstrated no to moderate change in post-test probability for the diagnosis of FAIS. Although low, SAE demonstrated a statistically greater mean diagnostic accuracy compared with the SCE (53.6% vs 45.5%, p=0.02).
Conclusion Diagnostic accuracy was statistically significantly higher for the self-exam than for the traditional clinical exam although the difference may not be clinically relevant. Although the mean accuracy remains relatively low for both exams, these values are consistent with hip exam for FAIS reported in the literature. Having established the validity of an SAE, future investigations will need to evaluate implementation in a telehealth setting.
- femoroacetabular impingement syndrome
- telehealth
- diagnostic accuracy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
A patient’s self-performed examination was more accurate for the diagnosis of femoroacetabular impingement syndrome than a traditional examination performed by a clinician.
How might it impact on clinical practice in the near future?
These data establish the validity of a patient’s self-performed examination that may be implemented into a telehealth model to help improve early diagnosis of hip pathology and streamline access to care.
Introduction
Telehealth has become an increasing subject of study due to the potential for providing equitable access to care1–3 and improving triage to the appropriate providers.4 5 The integration of telehealth into clinical practice may also have economic benefits, contributing to improved costs of care.5 The clinical exam provides key diagnostic information to support accurate diagnosis and decision-making in musculoskeletal care. Effective and comprehensive telehealth approaches to musculoskeletal care must evaluate the marginal impact on diagnostic accuracy of and/or reproduce this element of the evaluation approach. A patient-performed screening physical examination may offer a solution; however, the diagnostic utility of such an examination must first be evaluated.
Although the number of arthroscopic hip surgeries for intra-articular pathology continues to increase, accurate diagnosis of patients with hip pain remains a diagnostic challenge.6 7 Increasing focus has been placed on the role of clinical examination in the differential diagnosis of intra-articular and periarticular sources of hip pain.6 8 9 This is of particular interest given variability in the diagnostic accuracy of radiographic testing10–13 and the associated costs and barriers in access associated with such studies.
The primary objective of this study is to measure the diagnostic accuracy of a patient self-administered examination (SAE) of the hip versus a traditional standardised clinical examination (SCE) for diagnosis of femoroacetabular impingement syndrome (FAIS). A secondary objective was to evaluate the individual diagnostic accuracy metrics of both forms of examination and evaluate their influence of post-test probability of FAIS. FAIS was selected because of its relatively high prevalence, increasing diagnosis and surgical prevalence, and questionable examination utility in comparison to reference imaging. We hypothesised that there would be no difference in diagnostic accuracy between the patient-administered SAE and the clinician-performed SCE.
Methods
Study design
This was a prospective, case-based, case–control study design. The Standard for Reporting Diagnostic Accuracy guidelines were used in development of the methodology.
Participants
Following institutional review board approval, 80 patients seeking care from a fellowship-trained hip arthroscopy specialist for hip-related pain or mechanical symptoms were recruited for participation in an outpatient clinical setting. Consecutive patients were identified in an outpatient clinic of a tier-one institution from July 2017 until March 2018. Five patients were unable to complete the entire examination due to time constraints. The final number of participating subjects was 75. Testing was performed in the same outpatient clinical setting for all subjects. All patients underwent both SAE and SCE and were randomised to the order of the examinations.
Inclusion criteria
Ages 18–80 years; seeking care for hip-related pain and/or clicking, catching, giving way or stiffness, able to sign or verbalise study consent, without confounding medical conditions (eg, gynaecological or urinary pathology) and English speaking were approached for inclusion. No subjects declined.
Exclusion criteria
Patients with known lumbar spine or sacroiliac pathology, previous hip surgery, previous hip injury that would normally exclude from examination as standard practice, or inability to sign or verbalise consent were excluded.
Index tests
Subjective patient history
Based on a review of the literature for subjective findings associated with periarticular and intra-articular hip pathology the following subjective patient history items were collected prior to patient testing: location of pain included groin versus lateral hip,14–18 difficulty with stairs,19 20 pain with placing or removing shoes in a sitting position,21 pain with sleeping on one’s side, stiffness in the morning, pain in the morning, pain with sitting and ‘catching’ or ‘clicking’ in the hip.
Patient SAE
A review of the literature was performed to identify a series of self-performed manoeuvres associated with periarticular and intra-articular hip pathology (see table 1 for further details).21–25 Subjects met with the instructing provider in a private clinical exam room. The instructing provider was blinded to the final diagnosis. Reproduction of concordant pain (ie, pain consistent with that typically experienced by the patient) was considered a positive result for SAE manoeuvres.
Self-administered examination (SAE)
Standardised clinical examination
A literature review was performed to identify a series of clinician-performed examination manoeuvres to develop the SCE (see table 2 for further details).6 15 21 24–26 This standardised examination protocol was conducted by a different provider from the SAE. The examination included tests of passive range of motion and specialised provocative manoeuvres (eg, flexion adduction internal rotation (FADIR)) to assess for intra-articular pathology (table 2). Providers performing the SCE were blinded to the administration and findings of the SAE and vice versa.
Standardised clinical examination (SCE)
Reference standards
A diagnosis of FAIS was defined according to the Warwick Agreement which includes the presence of hip pain, clicking, catching or stiffness which is reproduced with impingement testing in the presence of cam or pincer morphology on plain radiographs in the absence of radiographic osteoarthritis (Tonnis grade 0 or 1).27 A diagnosis of osteoarthritis was defined as the presence of hip pain, clicking, catching or stiffness in the presence of radiograph findings of joint space narrowing, osteophyte formation and/or subchondral sclerosis/cyst formation (Tonnis grade 2 or 3). A diagnosis of trochanteric bursitis was defined as primary pain localised to the lateral hip, over the greater trochanter and reproduced with palpation.
Power analysis
The study is powered for the primary objective of the study, which is to measure the diagnostic accuracy of a patient-performed clinical examination versus a standard clinical examination. We powered the study by expected cell frequencies for those with and without an intra-articular disorder. Our previous works28 have shown a higher percentage of ‘True Positives (TP)’ for the intra-articular group (than false negatives (FN)) and we hypothesise a slightly higher percentage of true negatives (TN) than false positives (FP). With a projection of the following proportions, TP=47%, FN=20%, FP=13% and TN=20%, we would require a sample size of 75 to meet statistical significance.
Statistical analysis
Analysis was performed using SPSS (IBM V25.0). Diagnostic accuracy measures of sensitivity (SN), specificity (SP), positive likelihood ratio (LR+), negative likelihood ratio (LR−) and post-test probabilities were calculated for each component of the SAE and SCE.
SN was defined as the ability of the test to identify a positive finding when the targeted diagnosis is present, that is, TP. SP was defined as the ability of the test to identify a negative finding when the targeted is negative, that is, TN. LR+ indicates a shift in probability favouring the existence of a disorder if the test is found to be positive. Value greater than 1 indicates greater diagnostic strength. LR− indicates a shift in probability favouring the absence of a disorder if the test is found to be negative. Value less than 1 indicates better ability to determine a negative result. Post-test probability indicates a shift in the probability of the condition being present or absent relative to the pretest prevalence.
Diagnostic accuracy ((TP+TN)/(TP+TN+FP+FN)×100) for each examination was calculated and pooled for the SAE and SCE. Mean diagnostic accuracy was then compared using a Mann-Whitney U non-parametric test. A Mann-Whitney U test is the non-parametric alternative equivalent to a t-test but is a more conservative measure that does not require the same assumptions as a parametric test of differentiation. A statistically significant finding was defined as p<0.05.
Missing data
Complete data were available in 97.6% of test items. In total, 92.5% of the individuals had complete cases. Because the missing values were limited and consisted primarily of categorical values, SPSS was instructed to skip missing values during statistical analysis, despite values being missing at random.
Patient and Public Involvement
The development of the above described methods was designed to cause the least possible amount of disruption to the patient’s clinical experience. Although patients were not directly involved in the development of the study protocol, outcome measures were developed based on the patients’ subjective experience. The results of the present study will be disseminated to patients to whom Telehealth care is offered as deemed appropriate in the clinical setting.
Complete data were available in 97.6% of test items. In total, 92.5% of the individuals had complete cases. Because the missing values were limited and consisted primarily of categorical values, SPSS was instructed to skip missing values during statistical analysis, despite values being missing at random.
Results
For the 75 included patients, mean age was 45 (range 18–77) with mean body mass index of 28 (range 17–68). Regarding self-reported gender, subjects were 67% female, 33% male. Regarding self-reported racial identity, subjects were 73% White/Caucasian, 13% Black/African-American, 3% Asian/Native Pacific Islander with 9% declining to report. Regarding self-reported ethnicity, subjects were 88% non-Hispanic/Latino, 1.5% Hispanic/Latino with 11% declining to report.
Online supplementary appendix 1 outlines the SN, SP, positive and negative predictive values, LRs and accuracy values of the SAE and SCE. In general, the CIs of the LRs were wide for each of the tests, with a majority crossing 1.0. A number of the tests had diagnostic accuracy results below 50%. The FADIR test had an overall accuracy of 70.11% and demonstrated statistically significant increases and decreases in post-test probability. Pain with palpation of the lateral hip was also statistically significant and had an overall accuracy of 64.37%. The largest change in post-test probability for a statistically significant test involved the FADIR test, with a negative finding decreasing post-test probability by 30%.
Supplemental material
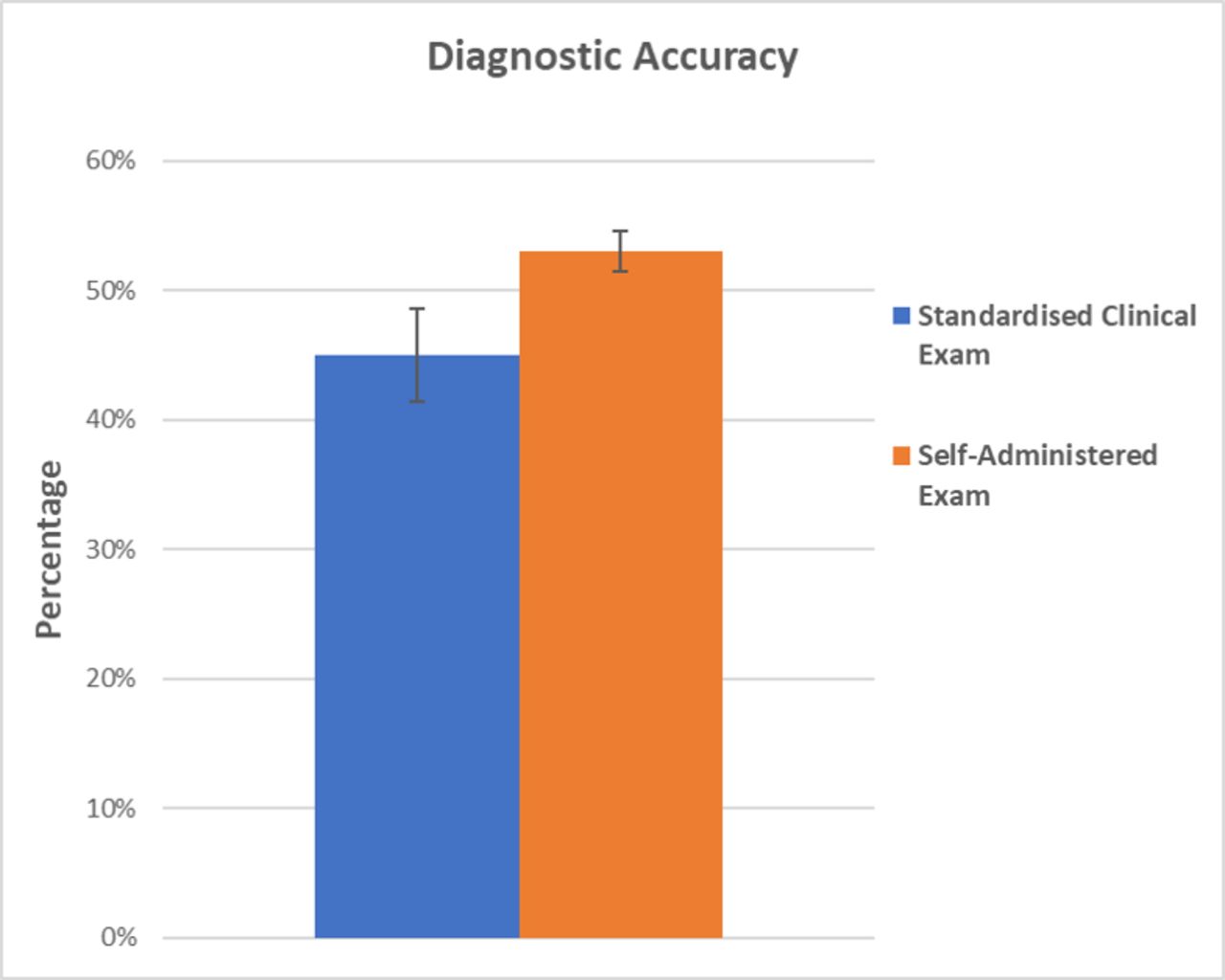
SAE demonstrated a statistically greater mean diagnostic accuracy compared with the SCE (53.6% vs 45.5%, p=0.02) (figure 1). The diagnostic accuracy of individual SAE manoeuvres varied widely.

{kind=link}
Comparison of the two testing formats demonstrated a significantly higher diagnostic accuracy for the self-administered examination (53%±1.6%) versus the standardised clinical exam (45%±3.6%). P=0.02.
Discussion
The present investigation demonstrated three notable findings which we believe merit explanation and further study. First, the diagnostic accuracy of a patient SAE for FAIS was statistically higher than that of a traditional clinician-performed examination. Second, neither examination protocol demonstrated a strong diagnostic accuracy or influenced post-test probability of diagnosis for FAIS in an outpatient orthopaedic surgery clinic. Third, the results of the SAE may be transferrable to a telehealth setting; however, further investigation is needed first.
Previous investigations have evaluated the diagnostic accuracy of physical examination for intra-articular hip pathology. Notably, in a meta-analysis of 21 studies evaluating the diagnostic accuracy of physical examination for FAIS, Reiman et al demonstrated minimal increase in post-test probabilities for physician-performed physical examination.28 An earlier systematic review performed by Tijssen et al also illustrates the diagnostic complexity of FAIS, ultimately finding none of the examination manoeuvres evaluated to be reliable for confirmation or disagreement with diagnosis.29 These findings may be related to the practice setting in which these examinations are performed. Once a patient has been referred to the outpatient clinic of a hip arthroscopy specialist, there is a high potential for verification bias by the provider which may dampen the effect of physical exam on final diagnosis.
The difficulty with consistent diagnosis of FAIS may relate to the relative heterogeneity of the condition. As a syndrome with multiple described subtypes (ie, cam, pincer, mixed), a large variety of patients with potentially very different presentations may fall under the diagnostic umbrella of FAIS. This may be reflected in the heterogeneity of the present study’s findings. Several examination manoeuvres when evaluated individually did demonstrate an improvement in post-test probability; however, this effect was diminished when the results were pooled. Given these findings, further evaluation of specific clusters of exam manoeuvres is merited to potentially elucidate the most reproducibly accurate tests for diagnosing providers. A cluster analysis also can further narrow the number of self-exam manoeuvres to improve the ease of implementation and evaluate how these manoeuvres relate to the different subtypes of FAIS.
In addition to further cluster analysis, future directions will analyse the effect of intra-articular injection on the predictive value of our examination protocols. A recently published investigation demonstrated that in situations of low disease prevalence and low examination sensitivity, diagnostic injection was more beneficial than advanced imaging.30 Further economic and decision model analysis is merited to determine the optimum combination of examination manoeuvres and diagnostic injection in the diagnosis of FAIS. This line of study will be further expanded to evaluate the effect of these diagnostic measures on the ultimate decision to proceed with surgical intervention.
Given the ever-expanding population and the physical limitations of providers, telehealth represents an opportunity to expand access to care and facilitate appropriate triage of patients. In concept, telehealth has shown increasing acceptance among providers and patients. A recent cross-sectional analysis of patient satisfaction for 3303 individuals demonstrated that the majority of patients were very satisfied with their telehealth experience.31 It should be noted that the cost-effectiveness of telehealth remains controversial, with several investigations demonstrating a lack of cost savings compared with traditional care.32 33 Notably, those controversies appear to be most prevalent with regard to treatment of long-term or chronic conditions. In the orthopaedic setting, telehealth application has been associated with reduction of cost, time and hospital visits following major joint arthroplasty34; however, the capacity for accurate diagnosis remains controversial.35 36
At this time, further investigation is merited into the effect of telehealth on utilisation and cost in the more acute orthopaedic setting. We envision a two-phase approach with the first phase being to assess accuracy of both the clinician-administered and patient-administered exam and the second to evaluate implementation of the SAE in a telehealth setting. Important questions include when and how the patient should perform the exam as well as the accuracy in practice. The present study satisfies phase 1 by establishing a proof of concept for a patient-performed examination to diagnose FAIS. The above stated future directions of study may help establish a feasible set of examination manoeuvres that may be performed remotely by patients with hip pain via a telehealth model.
Limitations
As discussed above, neither SAE nor SCE demonstrated a strong influence on the post-test probability of FAIS diagnosis. Within each group, there was a large degree of variability with regard to accuracy measures evaluated. This may relate to the high degree of variability among patients with a diagnosis of FAIS. For the present investigation, the reference standard for evaluation of accuracy was clinical diagnosis of FAIS based on interpretation of radiographs and clinical impression. Although the Warwick Agreement on femoroacetabular impingement27 was used as a guideline for this reference, this method introduces an element of potential bias. Finally, the demographics of the included subjects are not representative of the larger population, potentially limiting our ability to generalise the results of the present study. Having established the proof of concept, future study directions will include cluster analysis of specific sets of examination manoeuvres to evaluate for high-performing tests to be used in clinical practice.
Conclusion
A patient SAE for FAIS demonstrated higher pooled diagnostic accuracy than a traditionally performed provider examination. Having established a proof of concept, future directions will investigate potential implementation of patient self-examination in a telehealth model.
References
Footnotes
Contributors All listed authors were integral to the planning, execution, writing and revision of the present study. All coauthors contributed substantially to the study design, acquisition, analysis and/or interpretation of data. Final approval of the submitted manuscript was obtained from all coauthors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional review board approval was obtained prior to initiation of this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.